This week I talked with some folks at Glycom, based in Denmark. I had made contact with them because of seeing a post from someone stating their product “2-FL” resulted in them no longer being histamine sensitive. Histamine issues are very hard to deal with, see this post. This product is not for sale in the US. BUT there is a clinical trial for IBS (Rome IV Criteria ) (opened on May 14th, 2018), Effect of HMOs as Nutritional Support for Normal Bowel Movements in IBS Patients (GRIPS) <– this is the link to the official page
What is HMO?
It’s Human Milk Oligosaccharides — to be more precise, bio-identical oligosaccharides which would be found in mother’s milk. We all know that a child that is breast fed usually grows up with less health problems than a bottle fed one.
You may know of and benefited from whey, prebiotics etc. HMO is a magnitude above this! IMHO (could not resist the play of letters).
Read the Study yourself
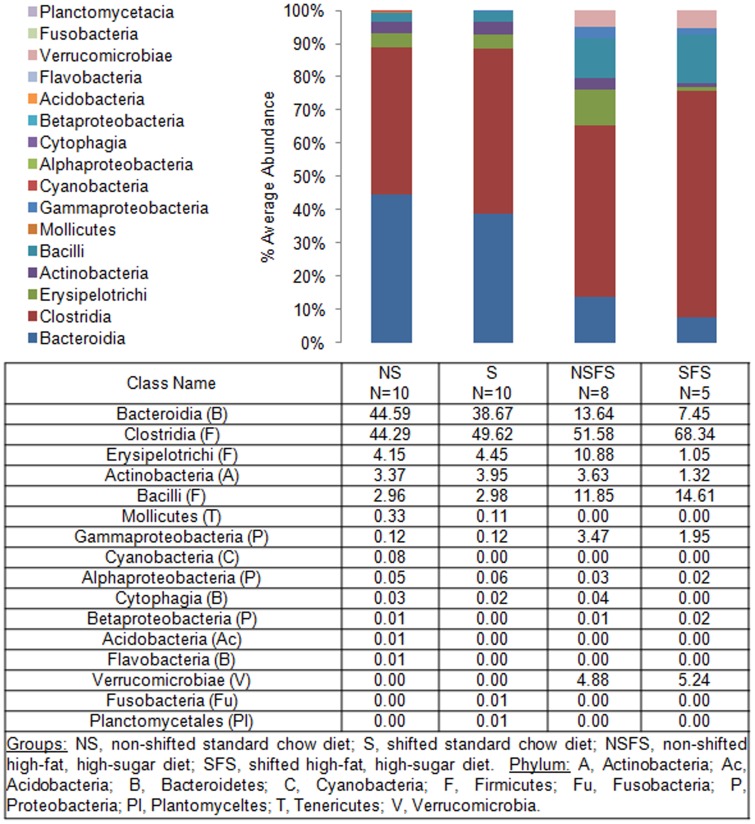
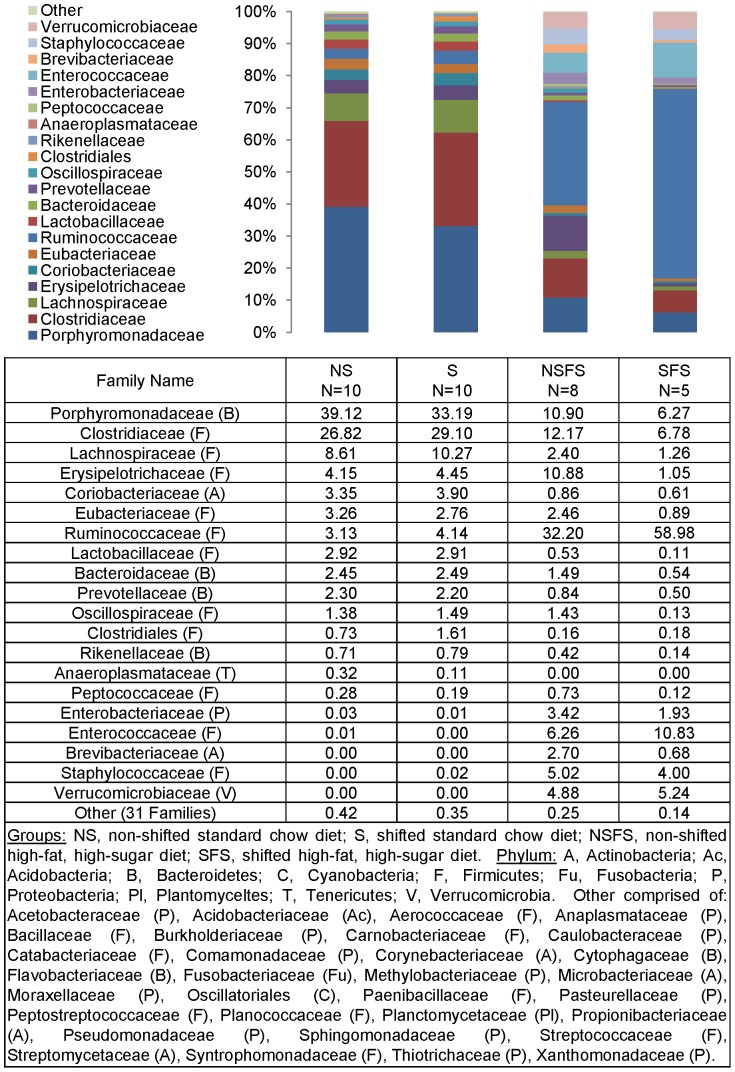
“Oral supplementation of healthy adults with 2′-O-fucosyllactose and
lacto-N-neotetraose is well tolerated and shifts the intestinal microbiota” Oct, 2016
This was over 2 weeks only — this trial is for 12 weeks!
- “showed that HMO supplementation specifically modified the adult gut microbiota with the primary impact being substantial increases in relative abundance of Actinobacteria and Bifidobacterium in particular and a reduction in relative abundance of Firmicutes and Proteobacteria. “
- “HMO are probably best known for their prebiotic effects in breast-fed infants, where they exert a strong bifidogenic effect, characterised by the proliferation of specific strains including Bifidobacterium infantis, B. breve and B. bifidum”
You will be getting it — and not a placebo!
“This is an open labeled, one-armed real-world study in IBS-patients. All participants will receive active treatment for 12 weeks.” One armed means everyone gets it!
The name is Fuco-N-Tetraose, packaging is below

How do you get on this in Europe?
This trial does not involve clinical centers nor physicians. It is restricted to EU due to regulatory requirements. http://www.himoexperience.com/ That is, a european mailing address and european telephone number is required. There is no requirement for any condition (like IBS).
How do you get on it on this US Clinical Trial?
You need to be diagnosed (by your primary care person or other professional, i.e. a gastroenterologist) with irritable bowel syndrome (IBS) in accordance with the Rome IV criteria. What is this criteria?
Rome IV Criteria for Diagnosing IBS:c
Recurrent abdominal pain, on average, at least 1 day/week in the last 3 months, associated with two or more of the following criteria:
- Related to defecation
- Associated with a change in frequency of stool
- Associated with a change in form (appearance) of stool.
cCriteria fulfilled for the last 3 months with symptom onset at least 6 months before diagnosis.
Whom should you contact?
Catchca
You need to attend at one of the 20+ clinical centers involved once (listed below) — See User note at bottom for actual examples.
- New Windsor, NY
- Wyoming, MI
- Lancaster, CA
- San Diego, CA (2 Sites)
- Bronx, New York
- Miami, FL (3 Sites)
- El Cajon, CA
- Tulsa, OK
- Birmingham, AL (4 Sites)
If you have co-morbid MCS, Histamine or other allergies
Please, please try to join this trial!
All of these are the tough conditions to treat — if this works for even 30% of the people, it would be a major win for everyone.
- Chronic Fatigue Syndrome/CFS and IBS is fine.
- Fibromyalgia/FM and IBS is fine
- UC and IBS is not
- IBD and IBS is not
- IBS alone is fine
Update from a Reader
CLINICAL TRIAL OF PREBIOTICS (HUMAN MILK OLIGOSACCHARIDES) FOR IBS NOW RECRUITING IN US AND EU
I just started participating in a clinical trial for IBS.
It’s open to the public, in the US and Europe, for anyone who might be interested.
The three-month trial is for a prebiotic called Human Milk Oligosaccharides (HMOs). It is not yet available for purchase. The Danish manufacturer (Glycom) calls it Holigos, in the US, and HiMO, in Europe.
It’s a type of fiber — a pair of indigestible carbohydrates, in particular — found in human breast milk. The product is fermented from lactose derived from cow’s milk, but contains only trace amounts of lactose, in the end.
As I’ve discussed on the Fast Tract Diet — in my case, a diet that consists exclusively of ribeye, salt, water, and lemon juice — almost completely suppresses my IBS-D symptoms, but it does not appear to cure the underlying inability to digest carbohydrates, which is why I decided to participate in this clinical trial.
A phase 1 clinical trial of this product found that this product increased Bifidobacteria in healthy volunteers. Bifidobacteria are apparently instrumental in the gut’s ability to digest carbs.
The trial in which I am participating is phase 2, which is designed to test the efficacy of the product in sufferers of IBS.
However, please note that that page includes a few important errors:
1. It says, “You need to be within 50 miles of the 20+ clinical centers involved.” In my experience, that is not the case. I live 218 miles from the nearest clinical center. I was allowed to participate. I just had to drive 3.5 hours, each way, for a single office visit. Also, a friend of mine whose closest center is a plane ride away was told he could participate, if he was willing to travel to that center, for a single office visit.
C. If you live in the EU, there’s no need to contact anyone at all. Just fill out your information at
http://www.himoexperience.com, to receive the free product in the mail. As far as I can tell, you don’t even have to have IBS, to get it — just a mailing address and phone number in the EU.
For what it’s worth, I’ve tried both galacto-oligosaccharides (brand name: Bimuno) and colostrum, to no avail. In fact, they both made my IBS worse.
I’m slightly more optimistic about Holigos, but only slightly.
I’ve used Holigos — 5 grams per day — for three days, now. I’ve seen no improvement thus far. It does cause me a small bit of gas — which is to be expected, according to the phase 1 clinical trial, whose results you can read at
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5082288/ — but that’s the only effect I’ve thus far been able to discern.
There’s probably about two teaspoons of powder per sachet — 5 grams in total. Patients are directed to take one sachet per day. It tastes sweet, like dextrose — but not as sweet as table sugar. One can add it to food, water, or other beverages — or, if one prefers, just pour the powder directly into one’s mouth, as I do, to enjoy the sweetness in its maximum concentration.
Quotes:
Here are some key quotes from the aforementioned review article — “Human milk and related oligosaccharides as prebiotics” — regarding HMOs:
>Recent studies investigating the catabolism and fermentation of HMO by bifidobacteria show that some strains have unique preferences in oligosaccharide consumption. Genomic analysis of Bifidobacterium infantis and Bifidobacterium bifidum, two related strains that grow well on HMO, revealed distinctive gene clusters that are specifically induced during growth on these glycans [14,15]. These strains, typically found in breast-fed infants, reached higher cellular density when grown on HMO compared with their close relatives B. breve and B. longum bv. longum (typically found in adults). These results suggest that HMO may selectively promote the growth of certain bifidobacterial strains frequently isolated from breast-fed infants. Further studies on B. infantis identified clusters of genes associated with HMO import and consumption and revealed particular mechanisms that likely represent a competitive colonization strategy employed by these unique bifidobacteria [13,16]. HMO also enhance bifidobacteria persistence in the gut by increasing their binding to intestinal cells, as well as improving the integrity of intestinal barrier function via regulation of tight junction proteins [17].
>In addition, HMO containing fucose and sialic acid share common structural motifs with glycans on the infant’s intestinal epithelia known to be receptors for pathogens. As such structures are known to act as pathogen receptors, their presence in milk may provide a defensive strategy by acting as decoys to prevent binding of pathogens to epithelial cells [3,4].
*****
Here is a key quote from that article regarding bovine (i.e., cow) colostrum (i.e., the milk produced just after an animal gives birth):
>There are 40 unique BMO [bovine milk oligosaccharides] in bovine colostrum, including 24 acidic structures containing sialic acid, and 16 neutral oligosaccharide structures containing glucose, galactose and N-acetylglucosamine [20]. The identified oligosaccharides in bovine colostrum include several structures identical to neutral and acidic HMO, including lacto-N-neo-tetraose, lacto-N-neo-hexaose, 30 sialylactose and 60 sialylactose. Parallel glycoprofiling breakthroughs
also revealed that these neutral oligosaccharides were preferentially consumed by B. infantis in in vitro studies [25].
*****
And here are some key quotes from that article regarding galacto-oligosaccharides:
>Much has been made of the occurrence of GOS [galacto-oligosaccharides, such as those found in Bimuno] in human milk. In reality, human milk oligosaccharides (HMO) are a large and very diverse group of complex oligosaccharides composed of several monosaccharide residues, and show little overall similarity with commercial GOS products beyond the fact that they are built on a lactose core (Figure 1). GOS produced through the enzymatic conversion of lactose do not occur naturally in human milk. However, there has been considerable interest in GOS as a component of infant formula feeds [36]….
>Walton et al. [39] have fed Vivinal GOS to elderly volunteers and characterized the changes in the fecal microbiota using FISH. Volunteers had a significant increase in bifidobacteria which returned to baseline after feeding ceased. This change was not seen with the maltodextrin placebo. Bimuno GOS has also been evaluated in a comparative human volunteer trial at doses of 0, 3.6 and 7 g/day, and bifidogenic activity correlated with dose [35].
>Impact of GOS consumption on health
>GOS were shown to have a positive impact on immune function [41]. In a 24-week crossover study of 70 healthy older subjects (average age 64–80 years) fed Bimuno GOS or placebo, improvements in phagocytosis and natural killer cell activity were seen together with a shift to a more anti-inflammatory cytokine balance, with an increase in IL-10 and decreases in IL-1b, IL-6 and TNF-a [41]. Whereas these results can be considered as a positive effect on immunity, the impact on disease susceptibility or resistance was not determined. The same GOS product, however, has shown positive effects in traveler’s diarrhea [42]. One hundred and fifty-nine travelers to high diarrhea risk destinations were fed 5.5 g GOS or maltodextrin placebo daily over a two-week trip. The GOS resulted in a statistically significant decrease in diarrhea incidence from 38.5 to 23.5%. Decreases were also seen in duration of diarrhea from 4.6 to 2.4 days and in duration of abdominal pain from 3.5 to 2 days. Given the nature of traveler’s diarrhea, it was not possible to identify the causative agent in the diarrheal cases making it difficult to speculate on the likely mechanism of action. Conceivably this may involve stimulation in immunity as reported by Vulevic et al. [41].
>GOS has also shown potential to improve the symptoms of irritable bowel syndrome (IBS) [43]. In one study on 44 IBS patients fed 3.5 or 7 g/day GOS or 7 g/day maltodextrin placebo for twelve weeks, there were changes in fecal microbiota as determined by 16S-FISH, and there was a selective increase in bifidobacteria. Flatulence, bloating, stool consistency, anxiety and a subjective global assessment of severity were all significantly improved in the GOS fed subjects. Although the mechanisms of the effect are not established at the present time the authors draw parallels with a study on bifidobacterial probiotics where the probiotic normalized the aberrant IL-10/IL-12 ratio in peripheral blood of IBS patients [44].