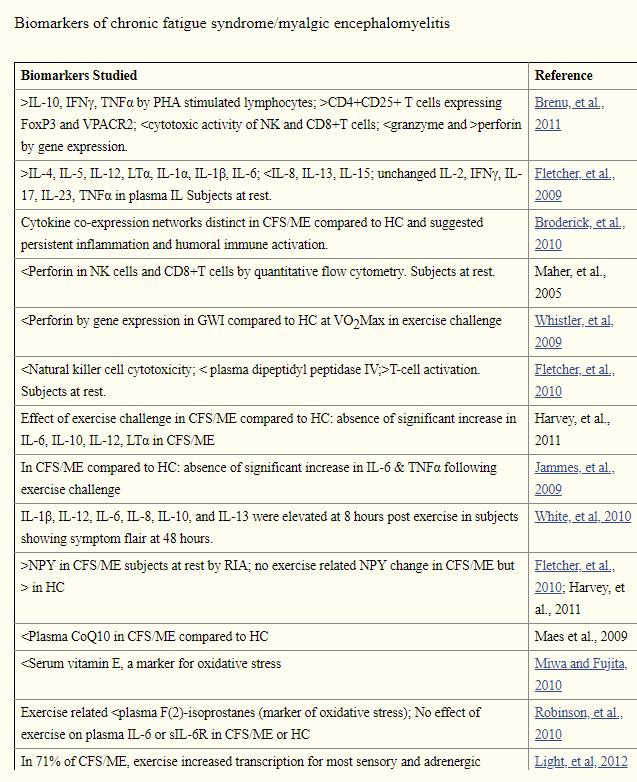
The same reader that asked about Biological Markers for CFS/ME, came back with a tougher question:
- “Now- another huge ask- have you written a post on the efficacy of various treatments? “
The core problem is the need to have proper control studies — which can be a challenge to both design and do. Often in reviews of the literature we will read issues like:
- poorly controlled sample populations
- too small sample size
- different studies types – observational studies (STROBE), clinical trials (CONSORT), or diagnostic studies (STARD or QUADAS),
My Assumptions
First, in the lack of better information — take things at face value. Suspend prior-beliefs and disbelief.
In my 1999-2001 episode, I reviewed all of the literature at that time and found two treatments that asserted over 50% success rate in publications or in presentations. I, with significant effort and patience, persuade my family practice physician to do both with me. These two treatments appear to be totally unrelated.
Rickettsia Protocol
This was resurrected by Cecile Jadin, a surgeon in South Africa, from attending meals with her father and his colleagues — they were researchers at the Pasteur Institute for Tropical diseases.
From her presentation at the Manly Conference (Australia): [Paper]
- 3 – 24 months of treatment (appropriate antibiotics pulsed)
- 8 months average
- maintain an 84% to 96% recovery rate (using the records of three MDs using it)
- Dr. CL Jadin – larger number than any below
- Dr. Phillipe Bottero – 100 patients
- Dr. Peter Tarbelton – 300 patients
Reality: Prescribing antibiotics per protocol will often place MDs in jeopardy with Medical Boards. I know of at least two that can no longer practise medicine because of this.
For an Actual Report see A reader report — 100% elimination of symptoms
Hemex Protocol
This was an accidental discovery by Dave Berg — who operated a speciality lab that dealt with testing for coagulation issues — typically for infertility due to Hughes Syndrome. He noted that many physicians using his lab mentions that patients with CFS reported their CFS symptoms disappeared while they were on low dosage heparin.
- “At the American Association of Chronic Fatigue Syndrome meeting, we presented a retrospective study of 20 patients looking at a hypercoagulable state that could be reversed with anticoagulant therapies” [1999 Article]
- “Dr. James Dey suggested that we do a retrospective study and even pulled out an abstract form for us for the American Association of Chronic Fatigue Syndrome. So we went back and looked at from between April and October, 21 cases that would be considered truly Chronic Fatigue patients and in that process, how did they improve?, what were their improvements like or was it a placebo effect?, and out of 21 patients, 19 had moderate to very good improvement and the other 2 at least had some improvement. ” [1999 Transcript]
- “In November, 1999, Dr. Joe Brewer (an Infectious Disease specialist in Kansas City) and I developed a model of pathogen activation of the immune and coagulation systems. The model proposes that the end result of such pathogenmediated activation is increased blood viscosity due to 1) an underlying coagulation regulatory protein defect, and 2) activation of the coagulation system by the pathogen. As the blood viscosity increases, the diminished blood flow creates hypoxia (lack of oxygen) and nutrient deprivation within various areas of the body. This is like trying to start your car in Wisconsin in the winter with 60- weight engine oil. This model explains the multi-organ symptomatology and also explains why the low dose heparin therapy is effective by increasing blood flow as the blood viscosity decreases. Thus, patients gain relief from their symptoms with this therapy.” [2000 Transcript]
- Improvement: 90% or better
Reality: The full panel of inheritable coagulation defects testing is rarely covered by insurance. Most MDs will not prescribe heparin, instead, refer patients to hematologists. Hematologists will see no clear coagulation events (i.e. stroke) and deem heparin is not warranted.
Heparin is a key component of the Hemex protocol.
Fecal Matter Transplants
From 2016 Review Article because IBS is so often co-morbid, I include those statistics.
- “fifty-patients with IBS and inflammatory bowel disease .. 36% remission, 16% subsided.”
- 45 IBS cases with the complaint of chronic constipation.. 89% immediate recovery, 42% remained in remission after 18 month
- 60 CFS cases .. 70% immediate… 58% remained in remission for > 15 years. 42% had remission disappear before 3 years.
Reality: In some countries (like the US), special permission must be obtained to do it. Identifying appropriate donors is still an evolving art.
Rituximab Treatment
“Øystein Fluge and Olav Mella of the Haukeland University Hospital in Bergen noticed its effect on CFS symptoms in 2004, when they used the drug to treat lymphoma in a person who happened to also have CFS.” – I have personally meet several people who went into remission from chemotherapy.
- “repeated rituximab treatment can keep symptoms at bay for years”[2015]
- 29 patients in study had 18 responders, remission over 3 years for 11.
- 62% chance of responding, if you responded, 61% of it lasting 3 years
Wish List: There have been zero studies on how rituximab alters the microbiome 😦
Bottom Line
All of the above successes fit perfectly into the microbiome dysbiosis/dysfunction model — including hypercoagulation ( Gut-derived endotoxin stimulates factor VIII secretion from endothelial cells. Implications for hypercoagulability in cirrhosis 2017). and Purinergic signaling during intestinal inflammation (2017). “Heightened thrombosis, inflammation, and immune disturbances as seen in IBD appear to be associated with aberrant purinergic signaling.”
Two of the 4 items clearly alters the microbiome. One deals with the symptoms caused by the dysbiosis — and the last one, may alter the microbiome (very probable)