I am working on a post on MCS and the microbiome. If you have MCS, uBiome results and willing to share your login for a week, please email me at Ken [at] Lassesen.com. During one episode with CFS, I had mild MCS which resolved with remission — this cause me to suspect that there is a significant microbiome aspect to this condition.
Patient Profile
- CMV epidemic and a mono-like illness may have been the triggering event
- IBS for 20 years, disappeared 14 years ago (may have been replaced by MCS 😦 )
- CFS for 25 years
- MCS for 15 years
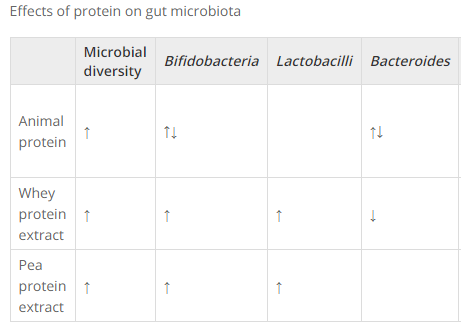
“I have improved from whey (Immunocal, ImmunoPro / VitalWhey), especially in MCS, begun at age 47. It is the only substance that has ever impacted the MCS. In terms of the CFS, however, I feel whey is propping me up to be capable of the minimal activity involved in taking care of myself, but that it is not curing. It feels as if I am gradually running out of steam.”
“In 2014, I tried:
- Neem leaf (abandoned after two days: gut distress, migraine, and intolerable hangover);
- Gerber Soothe Colic Drops L. reuteri (abdominal pain, gas);
- Securil Propio-Fidus P. freudenreichii (migraines, smelly poop);
- Ultimate Flora RTS Colon Care bifidobacteria (no clear result).”
Standard Checks
Doing my standard verification (pattern reported since 1998!):
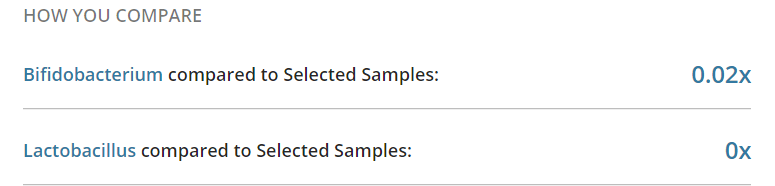
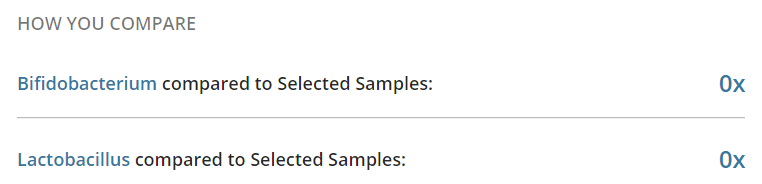
- Zero Bifibobacterium
- Zero Lactobacillus
- Zero Akkermansia (none reported)
- E. Coli is very likely zero
- Class: Gammaproteobacteria: 2% of normal
- Order: Enterobacteriales None reported
- See this post on Enterobacteriales levels on other uBiomes – 15 had very low or none.
- Diversity: 47%ile (i.e. “normal”)
Grand Slam!
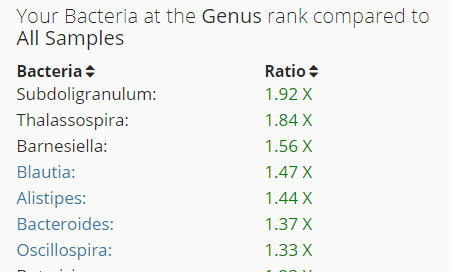
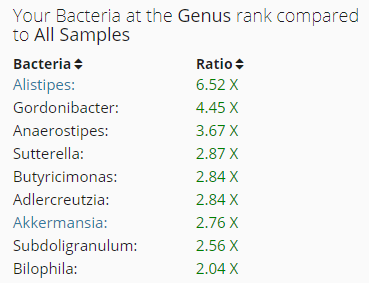
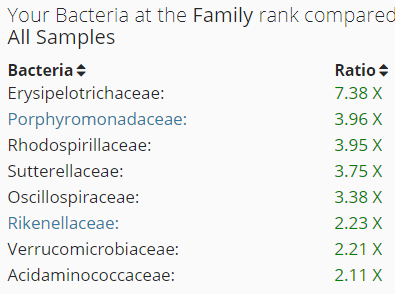
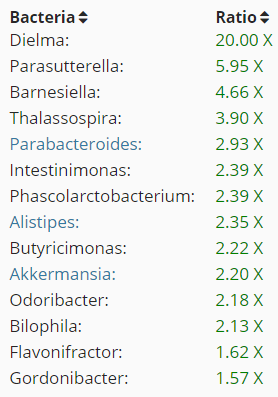
- There have been just 3 other uBiome with high Subdoligranulum.
- Two of them are also high in Thalassospira (with only 3 being high)
- None are also high in Barnesiella
- All are also high in Blautia (about 50% are high)
Analysis
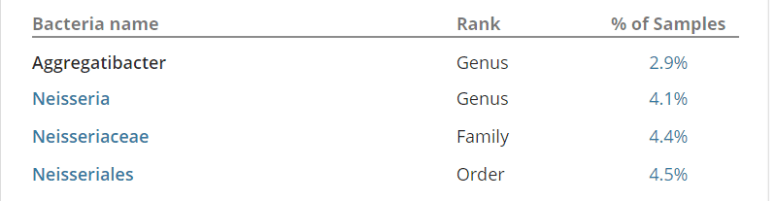
The Neisseriales order – we do not know it’s KEGG pathways (or much more about it) (from DataPunk). Only 1 other uBiome have any Neisseriales — based on the frequency of MCS with CFS, I would conclude that this is noise and is not MCS connected (and likely not CFS or IBS connected).
This leaves the following:
Looking at what is known to inhibits these
- Plant-rich diet – 5
- Tannin – 5
- Cranberry bean flour – 5
- Gallate – 1, 5
- Appears to be in some green teas
- Cranberry bean flour -5
Walnuts – 4- Flaxseed -4
And the flip side, enhanced (we do not want!)
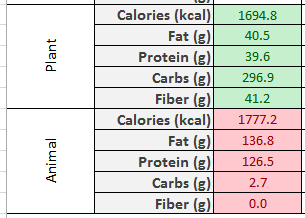
- High fat diet – 5
- High fruit intake -5
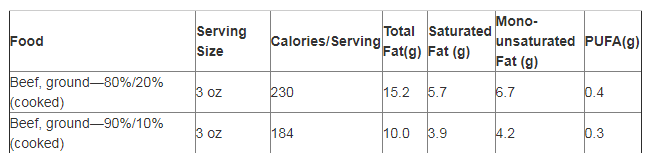
- High meat diet -5
Walnuts – 1, 4- Saccharomyces boulardii -1, 4
- Berberine -1, 4
- Bile -3
- Cholic acid -4
- Resistant starch (type IV) -4
- Resistant starch (type II) -4
All of these genus are known to inhibit bifidobacteria (note: some bifidobacteria are known to inhibit other bifidobacteria — it is not one happy genus!), and bifidobacteria is known to inhibit all of the above.
Suggested Initial course of action
The following are known to increase bifidobacteria (see link above)
- Sesame cake/meal
- Resistant starch (type III)
- Daesiho-tang (DSHT)
- Almonds/ almond skins
- Jerusalem artichoke
- Red wine
- Fructo-oligosaccharides
- Arabinoxylans
- Chicory
- Inulin
- Resveratrol
- Magnesium
- Chondrus crispus (red seaweed)
- Green tea
- Navy bean (Cooked)
Because of her issue cited above, I would suggest the following moderate change of daily diet:
- Green tea at least 3 times a day
- Magnesium Malate
- Resveratrol
- Almonds
BEWARE of Saccharomyces boulardii in yogurt and other products. You want to avoid.
Resistant starch: You want type III and to eliminate II (i.e. high amylose corn starch) and IV (“hi-maize resistant starch.”). See this post on another site.
I would suggest resuming with Ultimate Flora RTS Colon Care bifidobacteria, or other pure bifidobacteria products, see this post for relative costs. You may wish to try one box of Align (since it is a specific strain and is well documented). If the above goes well, then consider adding Prescript Assist or/and Equilibrium in.
As always, discuss changes with your knowledgeable medical professional.
Bottom Line
This is a long term CFS/MCS with a touch of IBS patient. who reacts adversely to several things. Altering diet to be unfriendly to overgrowth and supportive of undergrowth is likely a good starting point. Thanks to DataPunk, I was able to assemble lists of foods and supplements that are known to impact these bacteria.