A person who have done their uBiome several times over the last few years was kind enough to share their results. The numbers blew me away!!! If I had gotten a single lab with these numbers, I would suspect a lab error… but clearly that is not the case.
Standard Criteria
- Lactobacillus is typical very low
- Bifidobacteria is not — BUT if you look at the overgrowth, it is 1/100 (1%) compare to some overgrowth,,,
- Low or no E.Coli
- Not directly reported, but it parent is: Enterobacteriaceae which is 12% of the reference group
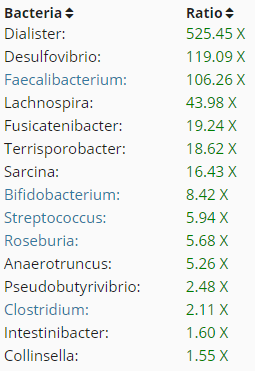
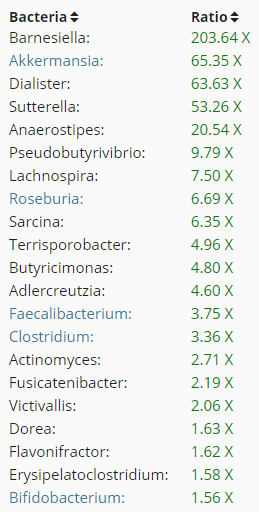
- High Akkermansia (parent is Verrucomicrobiaceae) 525% – 6500% of the reference group
Patient History
- Onset was in 2009 while living in a moldy apartment
- Trigger may have been wither H1N1 Flu or stomach bug overseas
- POTS, brain fog, PEM, Sinus, histamine issues
- Hypersensitive to mold
- Reacts mildly to fragrances
- No longer living in a mold environment
2013 uBiome
- Bifido: 2.27
- Lacto: 0.02
| 9/13/15 | 6/23/16 | 10/18/2016 | 6/13/2017 |
 |
 |
 |
 |
|
|
|
|
| This is using the latest results (6/13/2017). The number indicates the order in the results above. The data is from DataPunk.net
NUTRIENTS/ SUBSTRATES
INHIBITED BY
ENHANCED BY |
|||
NOTE: the comparison for Bifido and Lacto were against different references above.
Analysis
The above is a challenge. Please note that Lactibacillus (Genus) includes both Lactobacillus and Bifidobacteria. So the high number above is due to bifidobacteria.
I have worked only the current state — and included the known nutrients for these bacteria. My initial inclination is to starve them of the nutrients they need. D-Glucose which is blood sugar. This means going to NutritionData.Self.com listing high glucose foods and avoiding them. Some possible surprises for food to avoid:
- Apricots, Pineapples, Dates, Honey, Pomegranate juice, Grape juice… i.e. most fruits
- Pop, Melons, Squash, dill pickles, Cabbage, tomato products, radishes etc.
The person may wish to work with a nutritionist (if they can get their head around working on a low glucose diet — which is different from a low sugar diet. glucose is a specific type of sugar).
As shown above — walnuts, Saccharomyces boulardii and Proton-pump inhibitors (PPI) – are clearly to be avoided. While Flaxseed is on both inhibits and enhanced, it appears that it will inhibits a lot more than it enhances, and should be part of the daily diet. Flaxseed porridge with brown sugar for breakfast? (Brown sugar is sucrose, not glucose)
Bottom Line
The problem with many bacteria genus overgrowth is when to stop searching for a magical super set of supplements and food changes. My suggestion here is not to go on a low sugar diet (which will impact all bacteria), but a low glucose diet because the two biggest over growths feeds on this. This is some ways may be contrary to common sense health advice such as eating lots of fruits. You may wish to read wikipedia on glucose syrup (something to avoid)
As always consult with a knowledgeable medical professional (which may include a nutritionist) before any changes of supplements or diet. Keyword is knowledgeable…