Back around 1999-2002, the use of whey, colostrum and goat milk for CFS was popular. A friend was positive for EBV and after 2 months of an EBV specific colostrum, became negative. This was a pre-antibiotic treatment: You infect a pregnant cow with infection X and once the cow calved, you collect the milk which will high in antibodies programming against infection X. This method was far more expensive than antibiotics and did not scale well…. hence it was forgotten once antibiotics came along. Unfortunately, this EBV specific form of colostrum is no longer available.
“Colostrum and milk are rich in proteins and peptides which play a crucial role in innate immunity when transferred to the offspring and may accelerate maturation of the immune system in neonates.” [2005]
A reader asked about these, so a fresh look at the literature is done below.
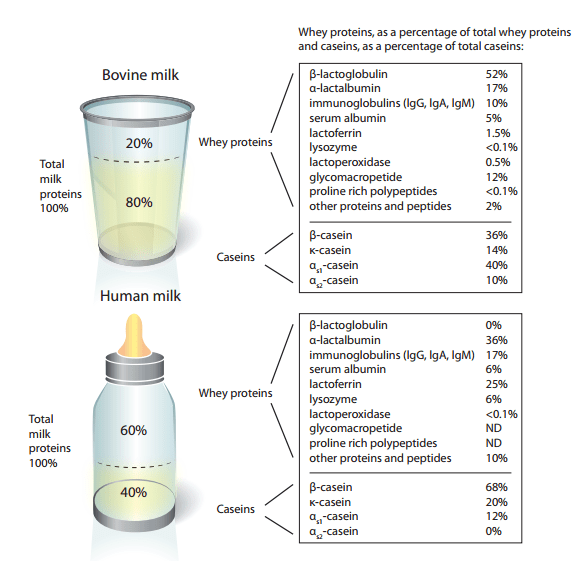
Human versus Cow Milk
The chart below illustrate well the difference [source]. They are VERY different.
Colostrum
“Colostrum (known colloquially as beestings,[1] bisnings[2] or first milk) is a form of milk produced by the mammary glands of mammals (including humans) during pregnancy. Most species will generate colostrum just prior to giving birth. Colostrum contains antibodies to protect the newborn against disease. In general, protein concentration in colostrum is substantially higher than in milk.” [Wikipedia]
It is heavily promoted in some alternative health circles [Example by a provider with citations to studies]
- Bovine antibodies targeting primary and recurrent Clostridium difficile disease are a potent antibiotic alternative.[2017]
- Milk-derived proteins and peptides in clinical trials.[2013]
- Molecular and biotechnological advances in milk proteins in relation to human health[2009].
- “Taken together, milk-derived proteins and peptides are bio-available and safe for the prevention and treatment of various disorders in humans and may play a complementary [natural agents] rather than a substitutional role to the toxic synthetic pharmacological drugs.”
- [Therapeutic properties of proteins and peptides from colostrum and milk]. [2005]
- “chewable tablets (Colostrinin) was recently found to improve or stabilize the health status of Alzheimer’s disease patients….In conclusion, preparations derived from milk and colostrum are effective, easily bioaccessible, and safe, finding wide application in prevention and therapy for newborns and adults.
- Treatment of multiple sclerosis with anti-measles cow colostrum. [1984] “
- “As a result, of 7 high NT titre (512-5120) anti-measles colostrum recipients 5 patients improved and 2 remained unchanged. Among 8 low NT titre (8-32) anti-measles colostrum recipients 5 patients improved and 3 remained unchanged. However, of 5 negative NT titre (less than 8) colostrum recipients 2 patients remained unchanged and 3 worsened. No side-effects were observed in colostrum recipients. These findings suggest the efficacy of orally administered anti-measles colostrum in improving the condition of MS patients (P less than 0.05).”
Whey
Whey protein is a mixture of globular proteins isolated from whey, the liquid material created as a by-product of cheese production. [Wikipedia]. As you can see from the figure above, why content varies according to source.
Back in 2000, “Non-denatured Whey” was a hot topic. “Undenatured whey protein isn’t heat-treated, so the fragile bonded cysteines that later form glutathione aren’t broken down in pasteurization.”[source] — so no pasturization (or homogenization) so the chemical structures of the whey are not damaged. At a philosophical level, this appears logical.
- “These findings indicate that the effect of heat treatment on whey proteins should carefully be investigated further.” [2017]
- Biochemical and clinical effects of Whey protein supplementation in Parkinson’s disease: A pilot study [2016].
- “This study is the first to report that Whey protein supplementation significantly increases plasma reduced glutathione, the reduced to oxidized glutathione ratio, BCAAs and EAAs in patients with PD, together with a concomitant significant reduction of plasma Hcy.”
- Limiting prolonged inflammation during proliferation and remodeling phases of wound healing in streptozotocin-induced diabetic rats supplemented with camel undenatured whey protein [2013].
- Camel whey protein enhances diabetic wound healing in a streptozotocin-induced diabetic mouse model: the critical role of β-Defensin-1, -2 and -3.[2013]
- Supplementation with undenatured whey protein during diabetes mellitus improves the healing and closure of diabetic wounds through the rescue of functional long-lived wound macrophages[2012].
- A whey-based glutathione-enhancing diet decreases allergen-induced airway contraction in a guinea-pig model of asthma.[2011]
- The biological activity of undenatured dietary whey proteins: role of glutathione [1991].
- “The presence in the serum albumin fraction of glutamylcysteine groups (rare in food protein) and the specific intramolecular bond as related to the undenatured conformation of the molecule are considered to be key factors in the glutathione-promoting activity of the protein mixture.”
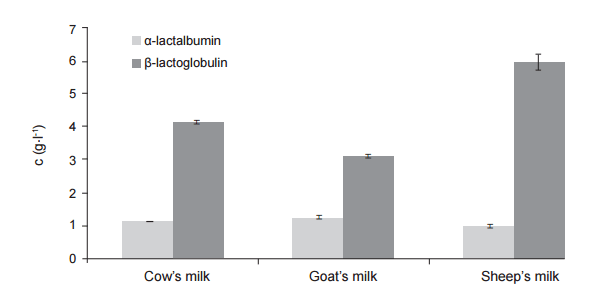
Other Non-Cow Milks
Looking at other milks, we find that Goat’s milk has less β-lactoglobulin (closer to human milk in a weak sense).
“Because an increase in the plasma Trp-LNAA ratio is considered to be an indirect indication of increased brain serotonin function, the results suggest that dietary protein rich in alpha-lactalbumin improves cognitive performance in stress-vulnerable subjects via increased brain tryptophan and serotonin activities.” [2002]
” The main components of whey proteins in camel milk and colostrum were similar to that in bovine, except for the lack in β-lactoglobulin.” [2007]
- Undenatured Goat Whey (Available from Swanson’s)
- Certified Organic Undenatured Bioactive Whey Protein (Swanson) – cheaper than ImmunoPro which was very popular in 2000.
- High alpha-lactalbumin whey Isolate is available (Davisco) [Product]
Bottom Line
There are no PubMed studies on whey and CFS/FM/IBS. There was one study for FM and one for IBS, one for CFS (by a questionable author – conflict of interests)
- “The objective of this clinical pilot study was to examine the induction of apoptosis in mononuclear cells on treatment of patients with chronic pain syndrome with oral immunoglobulin produced from bovine colostrum (BCC)….These results were accompanied by a relief of the pain symptoms [in 3 out of 4 patients]” [2009]
- “After 4 weeks (i.e. immediately after treatment), the endotoxin levels of [IBS] patients in the colostrum group showed a decrease in 44.4% (4/9) patients, no interval change in 11.1% (1/9) patients, and an increase in 44.4% (4/9) patients.” [2014] – helps some, makes other worst!
- Inconclusive (but positive) study for Gastrointestinal Infections[2008]
I would recommend trying them, especially the high alpha-lactalbumin whey Isolate because of it’s impact on cognitive function and also improvement of sleep. Please be aware that results are mixed — it’s a for better or for worst supplement.
I wish the infection specific colostrum were still available, and would love to see one specific for staphylococcus aureus [post].
“”