
My last post found some specific microbiome shifts associated with acid reflux. I thought that it would be good to revisit migraines (since the microbiome is getting more and more studied). My earlier post from a year ago is here (which includes probiotics suggestions). The amount of material is slim, but will likely increase in the next 2 years.
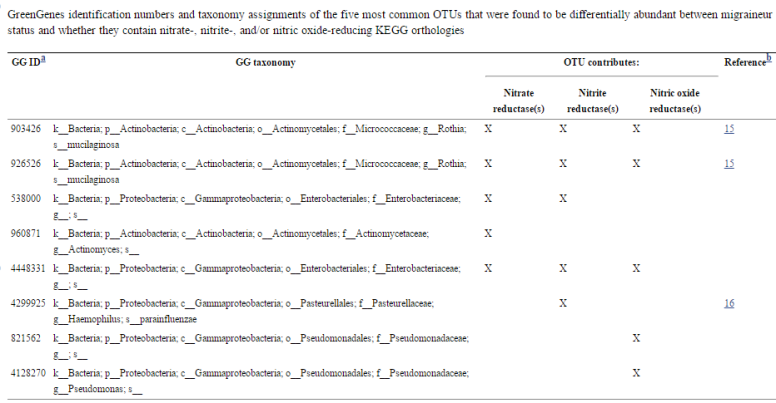
- Migraines Are Correlated with Higher Levels of Nitrate-, Nitrite-, and Nitric Oxide-Reducing Oral Microbes in the American Gut Project Cohort. [2016]
- “migraineurs share similar strains of Pseudomonas.”
- “two bacterial taxa (Rothia mucilaginosa and Haemophilus parainfluenzae) have previously been reported as some of the main nitrate reducers in the human oral cavity (12, 14), and some have also been reported to be associated with headaches (Table 1).”
- Migraines Are Correlated with Higher Levels of Nitrate-, Nitrite-, and Nitric Oxide-Reducing Oral Microbes in the American Gut Project Cohort.[2016]
- “The results of a small, non-randomized trial, including 29 migraine patients, showed a significant reduction in migraine severity after 12 wk of probiotic supplementation compared to baseline[104].”
- “supporting the idea that dysbiosis and altered assimilation of nutrients could have an important role in the physiopathology of migraine[105].”
Helicobacter pylori and the microbiome
Helicobacter pylori is seen in 40% of migraine suffers. This hints that it may be of interest to see what type of shifts is seen with it.
- “Within Proteobacteria, gamma- and beta-proteobacteria were the most abundant for H. pylori-negative patients, , whilst epsilon-proteobacteria was for H. pylori positive…In the H. pylori-negative patients, there was more relative abundance of Gamaproteobacteria, Betaproteobacteria, Bacteroidia and Clostridia classes ” [2016]
- “In H. pylori-positive patients, with respect to H. pylori-negative subjects, Maldonado-Contreras et al.28 report a higher abundance of Proteobacteria, Spirochetes and Acidobacteria; and a decreased abundance of Actinobacteria, Bacteroidetes and Firmicutes.”[2015]


