This is a follow up from a previous thread to show what type of information is available.
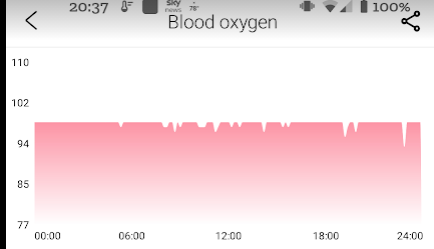
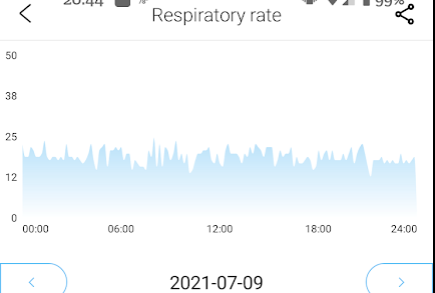
The $45 watch
The store is BangGood and the price varies. Today it’s $44, I had gotten it on sale for $32 earlier this year
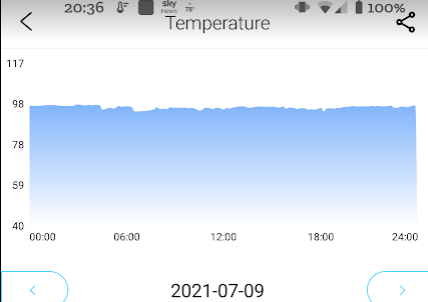
This is not “medical certificed”, but the numbers are good for on going monitoring. This watch can be set to record every 10 minutes of the day. Usually I need to recharge every 4 days with these constant readings
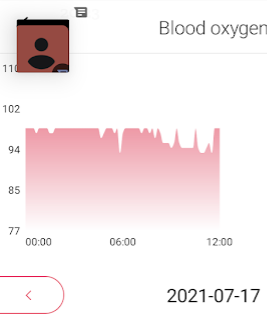
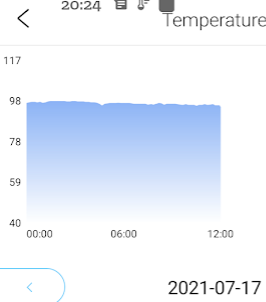
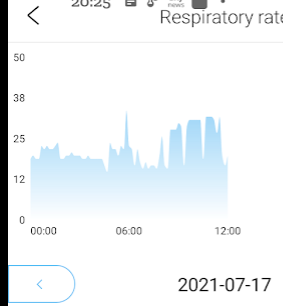
Example from the day that I got cellulitis
My watch was removed in the E.R. when I arrived at hospital, so only a half day was recorded. The charts illustrate the progression.
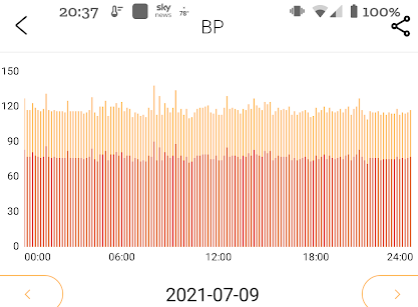
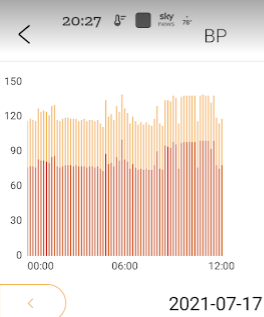
“White Coat Hypertension”
At my last checkup, the nurse reported high blood pressure… the BP chart agreed at the time she took my B.P. BUT it also showed that my BP is not high most of the time…..
A reader had initial success from modifying the microbiome but it did not persist.
The reason I ended up at your website doing research into the connection microbiome and ME/CFS was that firstly I tried Miyarisan and it turned out to be one of the best things I ever tried, MY headaches and brain fog were early completely gone and I had a lot more energy. Unfortunately this wonder only lasted about 6 weeks till I overdid it and crashed and with that crash Miyarisan lost it’s effect on me.
The other thing was Nystatin, which I was given for the candida found in my gut last year and right on from the first pills I took, it gave me more energy ( so I doubt it had anything to to with the candida, but rather must have changed something else in my gut for the better). This lasted about 10 weeks and then pooped out and was not reproducible.
But these two times that I felt I got energy because of some changes in my gut, were very rare in the way the they just generally provided a relief in all symptoms, as I was just overall feeling better and had more energy, but without crashing. Most of the times I have trouble, because I am easily overstimulated and most things that give me energy give me instant fatigue rebound, so Miyarisan and Nystatin really were different and made me try to work on my gut.
She attached her tests and summarized them as “As to my tests, I guess the most notable things are my low TH1(Interferon Gamma), my low glutathione, high TGF beta, my decreased SOD activity.”
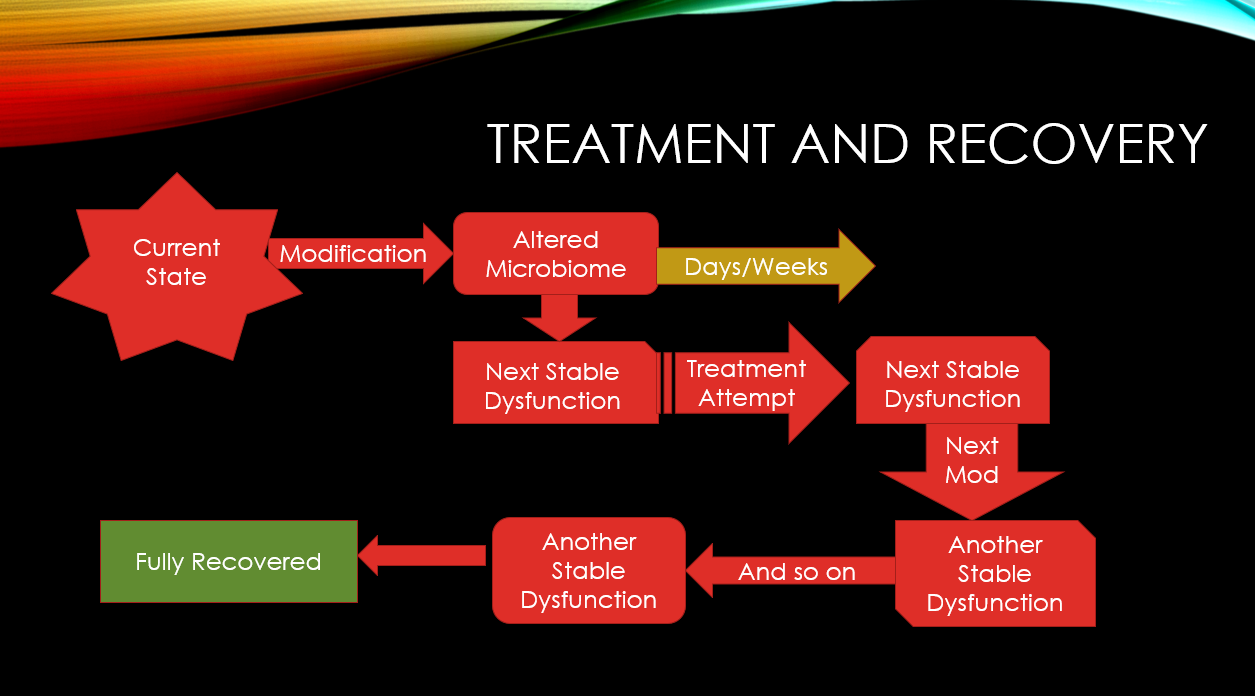
Reminder that recovery is a journey
In an earlier youtube review of another ME/CFS patient, I used the graphic below
I used this model for my last flare and can be seen by the list of posts below on CFS Remission. Each report was associated with a new microbiome test and a change of supplements etc to address the changes that the prior changes caused.
At this point we get some very interesting results. First, the bacteria by themselves do not match any symptoms.
But when we go over to the KEGG components that the bacteria produces, we see the type of predictions that we would expect
Conclusion: She does not have the typical ME/CFS bacteria shifts but she has the typical jacked metabolites imbalance seen in people with ME/CFS. Same crime — different crime family!
Action Plan
At this point, we have identify major items of concern.
Hand Picked Suggestions
I am going to run it two ways — first with the extreme outliers shown above, then including Firmicutes (which I rarely do)
If your physician is willing to prescribe “off-label” also do alternating every two weeks between a PPI and atorvastatin (prescription). PPI is over the counter in some places and includes:
omeprazole (Prilosec, Prilosec OTC, Zegerid)
lansoprazole (Prevacid)
pantoprazole (Protonix)
rabeprazole (Aciphex)
esomeprazole (Nexium)
dexlansoprazole (Dexilant)
For items from the suggestions above, I would suggest going with handpicked suggestion list without firmicutes.
I would suggest an initial retest at 4 weeks or so, a full cycle of a PPI and atorvastatin, at the same time a cycle of alternating licorice and triphala. We want to see if this has caused a downward movement of the two species of concern.
I am a strong advocate on doing alternative pulses. It is what C. Jadin does for antibiotics (changing them every month) and I also have read several modelling studies that found rotation had better success than continuous. The english explanation is simple: for anything you may take — 90% of the bacteria may be killed and 10% survive (resistant). If you keep up with the same, then that 10% slowly regrows as resistant to whatever you are using. Changing between two things that are 90% effective (and different), then it becomes 99% killed and 1% survive.
As you have witnessed, 6 weeks with one item and then the resistors recovered your dysfunction, for another substance it lasted 10 weeks. We want to keep to 2 weeks on and then rotate.
I checked the parent taxa on these two, and I see Carthamus tinctorius L (Safflower) inhibits one of them – so using safflower oil may help. There is no simple parent for the other.
As always, consult with your medical professional before implementing.
This is a two goal post. First, to see if literature indicating that healthy partners of microbiome dysfunction reflect their partner’s microbiome. Second, just a look at his microbiome and any possible concerns.
There is a very significant difference between the two in terms of diet:
Patient has been eating gluten free for years, supplements. etc
Husband eats gluten and dairy and some junk food. Minimal supplements. High lipids, possibly genetic.
Contrary to some studies, there appear to be little similarity between these people microbiomes. The reason is likely that the shifts due to diet are so very significant. It does raise the issue of using uncorrected ranges for diet types (junk food, organic, gluten free, vegetarian, pork eater, chicken eater [Yes, studies have shown difference between people that eat pork mainly instead of chicken!], etc.). Similarly age is a factor How the microbiome ages [2019]
Goal #2 Husband Health
As I know first hand, a wife usually cares more about a husband eating habits than he does himself. The risk of a kiss on the spouse cascading microbiome changes is a technical possibility.
First I went to Expert consensus
On the resulting screen, I checked all of the genus and species that were out of range and create a hand-picked selection and then got suggestions for them, shown below. Given that they are in the sixties, I note with interest that the first suggestion is the type of sugars found in mother’s milk, it almost seems to be a collection of restoring a younger microbiome suggestions.
Next I checked the Nat.Library of Medicine Explorer. To my delight, there were only two items above 50.
The items are:
hypertension (High Blood Pressure) — at 60%ile — still fine and not unexpected since hypertension is age related (likely connected to aging of the microbiome) see Hypertension – What we know [2019]
NonCeliac Gluten Sensitivity – This may be a false positive. Let me explained, since the wife is Gluten free, the husband will likely eat more gluten free food than most people. It you starve the gluten consuming bacteria… the shift may look like gluten sensitivity.
Going over to citizen science, there were no matches for symptoms. Again, compared to most people that have uploaded samples — no concerns.
Standard Kaltoft-Moldrup Suggestions
The suggestions are similar to those above. Many of the items are not unexpected for someone in the 60’s — Vitamin D. There is one significant change from above — resistant starch is a to Add, above, a common source of resistant starch (broad beans, black beans, etc) were on the to avoid list. Personally, I would go for eating the beans and other sources of resistant starch (see Resistant Starch Content in Foods Commonly Consumed in the United States: A Narrative Review [2020]).
High lipids – any known microbiome component?
I do not have lipids in the database yet, so the reader should review the following studies.
The husband seems fine and has no apparent health issues associated with the microbiome. There are suggestions above which may help prevent microbiome issues developing.
A reader asked me to review their microbiome and test results, for items to discuss with their medical professional. As always this is not advising what to do; suggestions should always be reviewed by your medical before implementing.
The Person
This woman developed CFS around Lake Tahoe in 1987. Lyme and Mold issues.
Resulting in MD prescribed Iron supplements, resulting in
23 lb gain (heaviest ever!) (fat gain)
High cortisol,
Insulin resistance,
Bloating
Antifungals and antibacterial herbs for the past 3 years for mold and Lyme. history of off and on antibiotics for Lyme and coinfections for decades etc.
Cytomegalovirus and Epstein Barr (common with ME/CFS)
Tried resistant starch(oatmeal and green banana) and my bad microbes tripled (unclear which ones were deemed bad)
Gluten-free for years
Food poisoning 5 years ago
Feels hypoxic (low oxygen to brain) – likely caused by Protein S deficiency that is part of the coagulation change (according to tests)
Genetic issues processing phenylene, leucine and lysine. And also oxalate issues
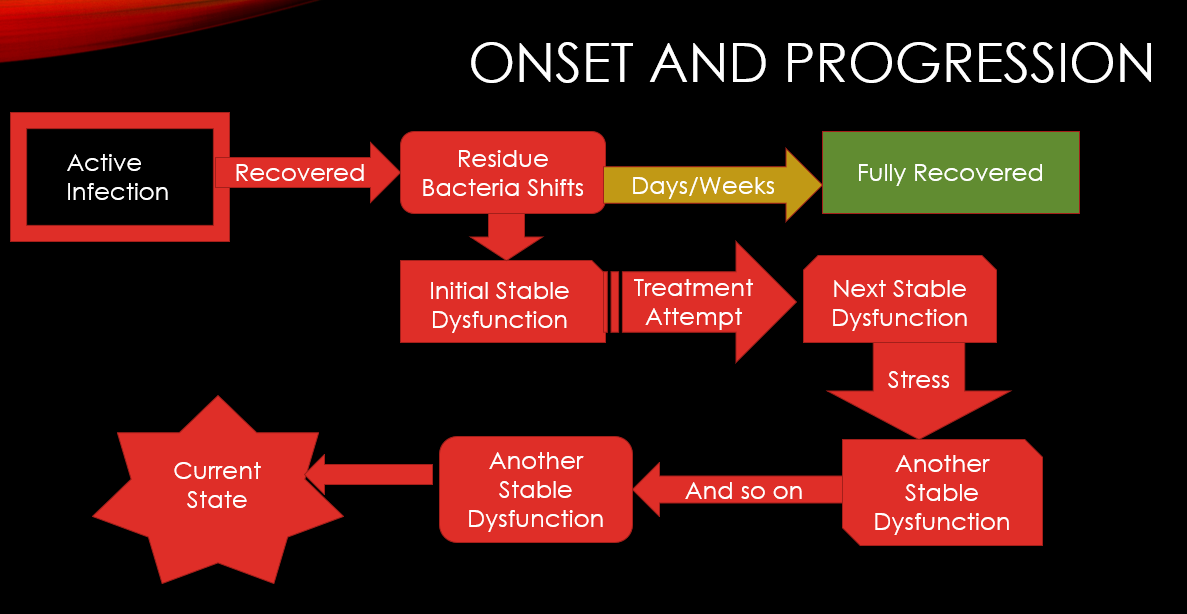
Markov Cascade Model
This chart shows how overtime the microbiome can recover or continue to cascade (evolve). It is not a one step change, it’s a series of changes over time caused by diet, treatment attempts, age etc. This is essential to understand why things change and that it is not a one-step recovery.
Over time, the stable dysfunction microbiome develops a unique evolutionPath to recovery can be many steps
The Samples
We have five samples from Dec 2020 until May 2021. Multiple samples is a short period of time allows the daily variation to be minimize. Due to age, we do not have to be concerned with time in cycle impacting her microbiome (a key factor for females doing comparison samples)
Initial Notes
Going to comparing multiple samples, I walked thru each of the outliers and jolt down concerns
No matches – this may indicate that the person has moved outside of the typical ranges
Building Suggestions
The numbers for the recommendations are among the highest that I have seen!!! This implies taht a lot of enzymes are not being produced. I would suggest the three easiest to obtain for a start, single Species with research (as shown below with the Books emoji)
For dosages, start low and slowly increase to the common therapeutic dosages
KEGG supplement list is long, even when reduced to just 3%ile
Amylase (Enzyme)
beta-alanine
D-Ribose
Glycine
L-Cysteine
L-glutamine
L-Histidine
L-Lysine
L-methionine
L-Serine
NADH
Selenocysteine
Prior to suggesting any of this list, i want to look at advance suggestions. The options that I picked
First, out of curiosity, given the experience with antibiotics, I looked at only antibiotics. Only a few of several hundred in the database made it on the possible list and at low confidence. The top 3 are often suggested with ME/CFS patients. the avoid list is massive. My impression is no antibiotics, but we need to confirm other paths are more probable to help.
I played with the other prescription options and the results were similar. So returning to the default suggestions we end up with an interesting list of do and don’ts
What makes it interesting is that a lot of to avoid are common suggestions from MDs treating ME/CFS with one-recipe fits all for ME/CFS. For example
Avoid all B-vitamins
No vitamin C
No Melatonin
No quercetin
Avoid Lactobacillus probiotics and likely bifidibacterium
The top item to avoid is luteolin. The foods that contain it are listed here and include celery seed, thyme, parsley, peppermint, rosemary and olives.
On the plus side I see my favorite ‘antibiotics herb’ being listed, triphala. Changing the diet to resistant starches and away from high gluten food. Care must be taken to make sure you do not destroy the resistant starch as shown below:
The reader is interested in antibiotics for fusobacterium. I usually try to discourage single-bacteria focus because side-effects on other bacteria may make the person worse. Often this approach leads to frustrations because things “did not work“.
We start by looking at the antibiotics (this link) where we find 103 different antibiotics that reduces it. Just below this section of the page we also see the bacteria that encourages or discourage; for her latest sample, none of these appear to be in play.
Looking at the suggestions for antibiotics only, and turning all the Show links to studies used for suggestions and setting the number of suggestions high, we see all antibiotics with probable positive impact, we end up with this list only.
We then click each link to see what each suggestion actually modifies, on #2, we encounter success. It reduces this bacteria AND increases a different bacteria in the wrong direction (Pediococus is TOO high). This illustrates the challenge of being focused on one bacteria.
Remember that we balance good and bad impact — so remember to check each items
There is no option to model what will probably happen. My goal is to increase the probability of a suggestion being helpful. This is a decision that the medical professional needs to make (ideally after being made aware of side-effects).
Bottom Line
This person is not the usual pattern with pretty extreme shifts in the microbiome. My suggestion for a course of action to discuss with your medical professional would be
reduce/eliminate any supplements/drugs not listed above for a month
shift over to the diet style above, with the few probiotics suggested
start at a low dosage of Triphala (we buy it organic bulk and make our own capsules) and increase it slowly to at least 2 grams/day, ideally 8 grams/day [basis of dosages]
To me the key thing is to simplify the influences on the gut and allow it to stabilize and then proceed from there with changes followed by re-test and a new set of changes.
I have often recommended Piracetam for cognitive issues. I have personally observed dramatic improvement within minutes in others, and observed it with myself. Unfortunately in the US it is not directly available because of FDA rulings (the same situation as for Mutaflor — E.Coli Nissle 1917 probiotic). Mutaflor is well documented (citations) with over 240 studies, and safely used in Europe for over a century — and works far better than any probiotic approved by the FDA.
Today, when I mentioned it, a facebook user wrote “Piracetam seems to come with warnings:” and linked to a JAMA article from 2019.
Our findings demonstrate that even after the FDA rejected an application to market piracetam as a new supplement ingredient,3 the drug was nevertheless introduced into the marketplace. Despite FDA warning letters,6 the products remain on the market. Until the law governing supplements is reformed such that products adulterated with drugs can be effectively removed from the market, clinicians should advise patients that supplements marketed as cognitive enhancers may contain prohibited drugs at supratherapeutic doses.
This was not a warning of the dangers of this substance — but a warning of the sale of a substancedirect to retail as a supplement ignoring FDA rulings in some products (which seems like a very American attitude 🙂 )
Originally marketed by UCB Pharma in 1971, piracetam was the first nootropic drug to modulate cognitive function without causing sedation or stimulation 1. It is not approved for any medical or dietary use by the FDA. In the UK, piracetam is prescribed mainly for myoclonus, but is used off-label for other conditions such as learning difficulties in children, memory loss or other cognitive defects in the elderly, and sickle-cell vaso-occlusive crises 4. Evidence to support its use for many conditions is unclear.
“Piracetam, a nootropic drug that has been clinically used for decades but remains enigmatic due to no distinct understanding of its mechanism of action. …. Piracetam treatment offered significant protection against LPS induced oxidative and inflammatory parameters and inhibited astrocytes activation. ” [2018]
The JAMA was concerned about supratherapeutic doses, i.e. above 1500 mg. Going over to DrugBank Pharmacology resource we read
The cases of overdose with piracetam is rare. The highest reported overdose with piracetam was oral intake of 75g which was associated with diarrhea and abdominal pain; the signs were most likely related to the extreme high dose of sorbitol contained in the used formulation
I suspect that the FDA ruling for piracetam is similar to that for Mutaflor. The decision was influenced by established american industries with a vested interest in selling their existing (ineffective often) products.























 Show links to studies used for suggestions and setting the number of suggestions high, we see all antibiotics with probable positive impact, we end up with this list only.
Show links to studies used for suggestions and setting the number of suggestions high, we see all antibiotics with probable positive impact, we end up with this list only.

