
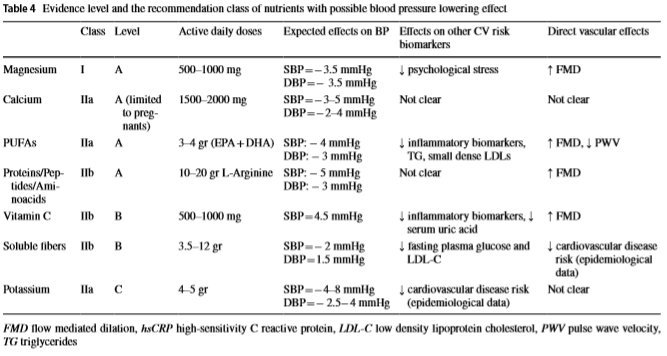
As we age, our ability to absorb magnesium, calcium and potassium decreases. Lower levels increases blood pressure.All three should be supplemented. And if you are prescribed medications for hypertension – they actually will drop these minerals lower and partially increases blood pressure. This is an awkward medication feedback — it contributes to what it is suppose to treat!
- Not enough minerals. Too little potassium, calcium or magnesium in the diet can cause leg cramps. Medicines often prescribed for high blood pressure can cause increased urination, which may drain the body of these minerals.“
https://www.mayoclinic.org/diseases-conditions/muscle-cramp/symptoms-causes/syc-20350820
As a result of my last post, several reader pinged my about hypertension, in some cases associated with POTS (a common morbidity with ME/CFS). This is just a quick recap of recent research.
The age-standardized prevalence of hypertension at baseline was 74.3% for men and 70.2% for women.
Prevalence and Incidence of Hypertension in the General Adult Population [2015]

Follow up 1 is 4 years later, 2 is 2 more years
- ” Obesity and weight gain also contributed to progression; a 5% weight gain on follow-up was associated with 20-30% increased odds of hypertension. ” [2001]
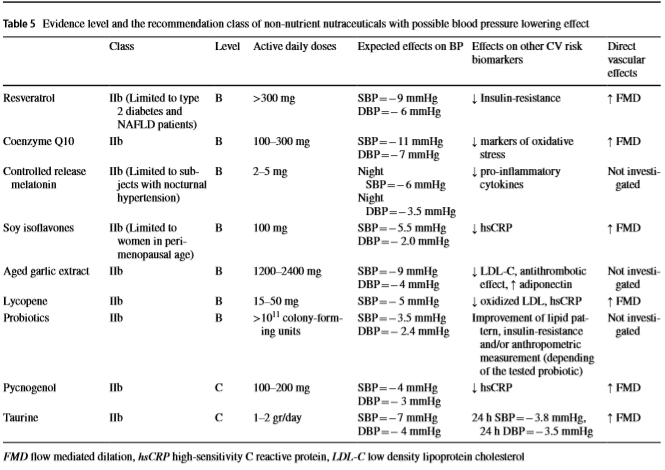
- “Dose-response analyses showed that all of the carotenoids[ β-cryptoxanthin, lycopene, lutein with zeaxanthin and total carotenoids ] were inversely associated with hypertension in a linear manner. Total carotenoids showed significant effect of lower risk of hypertension at 100 μg/kg per day. “[2019]
- ” It appears that the use of nutritional supplements and medical foods containing L-methylfolate and vitamin D may be effective in facilitating the improvement of diabetic and hypertensive retinopathy.”[2019] “
- ” In conclusion, higher dietary calcium intake, independent of adiposity and intake of other blood pressure-related minerals, is slightly associated with a lower risk of developing hypertension. ” [2019]
- Zinc deficiency is an independent risk factor for prehypertension in healthy subjects. [2019]
- ” When studies were categorized based on participants’ mean age, ginger dosage and duration of intervention, systolic BP and diastolic BP were significantly decreased only in the subset of studies with mean age ≤ 50 years, follow-up duration of ≤8 weeks and ginger doses ≥3 g/d. ” [2019]
- Cross-sectional NHANES data do not support the hypothesis of a positive association between choline intake and BP. [2019]
A nice summary article
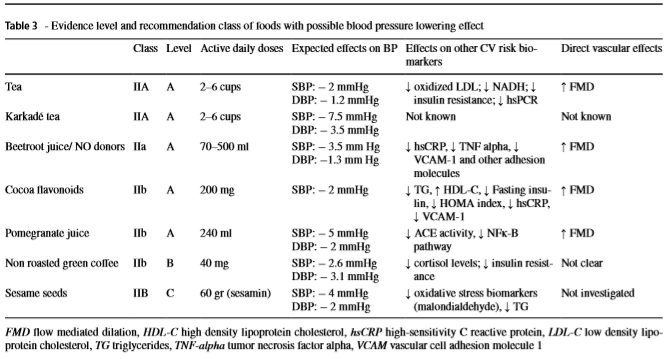
Other antihypertensives
That is, BP lowering substances, not cited above:
- Effect of hibiscus sabdariffa on blood pressure in patients with stage 1 hypertension. [2019] SBP: -7.4, DBP -6.7
- Flavonoids in hypertension: a brief review of the underlying mechanisms. [2019] ” catechins and quercetin impart significant blood pressure lowering effects “
- Ethnobotany of Anti-hypertensive Plants Used in Northern Pakistan. [2018] ” Pharmacological studies show that Allium sativum[garlic], Lepidium sativum [Garden cress], and Ocimum basilicum [Basil], Mentha sp.[mint], Trigonella foenum-graecum [Fenugreek], Urtica dioica[common nettle], Olea species [Olive], and Eucalyptus globulus[Tasmanian Blue gum] are effective species in treating hypertension “
- Antihypertensive Effects of Corn Silk Extract and Its Novel Bioactive Constituent in Spontaneously Hypertensive Rats: The Involvement of Angiotensin-Converting Enzyme Inhibition. [2019]
- Poor sleep quality increases blood pressure [2020]
- Consumption of nattokinase is associated with reduced blood pressure and von Willebrand factor, a cardiovascular risk marker: results from a randomized, double-blind, placebo-controlled, multicenter North American clinical trial. [2016]
- Effects of nattokinase on blood pressure: a randomized, controlled trial.[2008] SBP -5.55, DBP: -2.84
Earlier Posts
- Blood Pressure and the Microbiome
- Blood Pressure and CFS-IBS-FM
- CFS Low Blood Pressure, High Blood pressure and gut bacteria
- The Heart and Blood of the CFS Patient
Personal Observations
I have found that a combination of Piracetam with Bacopa Monnieri (and flushing niacin) dropped Systolic BP, mmHg by 40mm and Diastolic BP, mmHg by 10mm within 30 minutes. This effect lasted about 3 hrs.
- Bacopa Monnieri and Its Constituents Is Hypotensive in Anaesthetized Rats and Vasodilator in Various Artery Types [2011]
- Does nicotinic acid (niacin) lower blood pressure? [2009]
- [Effects of Piracetam on Occupationally Significant Functions of Patients With Arterial Hypertension Working Under Conditions of Psychoemotional Stress] [1995]
It is important to note that is may be just a transitory effect (i.e. a single daily dosage may not reveal significant changes in a study), that can occur on each dosing.
What is Piracetam?
Piracetam (2-oxo-1-pyrrolidine-acetamide), the most common of the nootropic drugs, is a cyclic derivative of gamma-aminobutyric acid [GABA]. The treatment with piracetam improves learning, memory, brain metabolism, and capacity. Piracetam has been shown to alter the physical properties of the plasma membrane by increasing its fluidity and by protecting the cell against hypoxia. It increases red cell deformability and normalizes aggregation of hyperactive platelets. Piracetam is an agent with antithrombotic, neuroprotective and rheological properties. The interaction of this molecule with the membrane phospholipids restores membrane fluidity and could explain the efficacy of piracetam in various disorders ranging from dementia and vertigo to myoclonus and stroke.
Piracetam–an Old Drug With Novel Properties? [2005]
Monitoring Blood Pressure
An upper arm pressure cup gives the most accurate results. I have also used a cheap chinese watch ($20) that records O2 saturation, Pulse and Blood Pressure every hour. The first two use the same technology used in clinics to get those two measurements. The Blood Pressure uses a different technology (more below).
Not all watches advertising Blood Pressure measurement support automatic hourly reading. Below is a screen shoot a few days after being released from hospital where an infection had pushed this to 160/110 for a while.
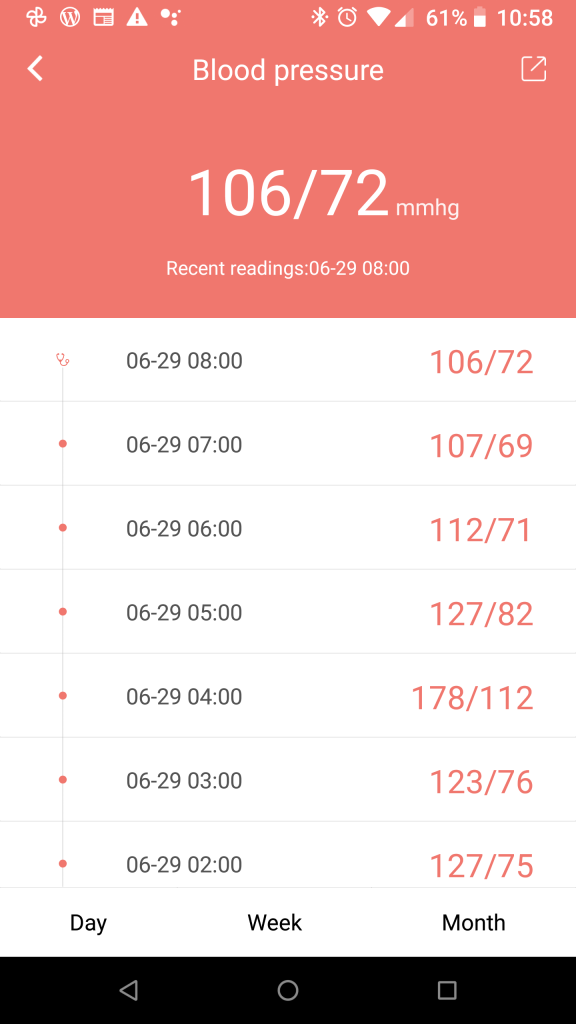
It is interesting that the mid-night spike at 4am appears to match with night sweats when I suspect that my body was fighting the residue infection. My pulse also went up to 159 (with 79 an hour before, and 85, then 64 after). O2 saturation also went up to 99% during this period. To me, not something of concern, just interesting.
UPDATE After a few months on the above

The watch is reasonable for general pattern only
” The accuracy guidelines were only met for the HR measurements in both devices. SBP measurements deviated 16.9 (SD 13.5) mm Hg and 5.3 (SD 4.7) mm Hg from the reference values for the Everlast and BodiMetrics devices, respectively. The mean absolute difference in DBP measurements for the Everlast smartwatch was 8.3 (SD 6.1) mm Hg. The mean absolute difference between BodiMetrics and reference SpO2 measurements was 3.02%.”
Accuracy of Vital Signs Measurements by a Smartwatch and a Portable Health Device: Validation Study [2020]
The high end Samsung watch has the same challenges. The technology, is described in this article The use of photoplethysmography for assessing hypertension [2019]. The measurements are still not up to par with upper arm cuffed blood pressure measure, with hopes for improvement over the next 5 years.
