I have often been asked that question. The general answer is “it depends”. This post gives you a science based answer.
Enter the probiotic Mixture
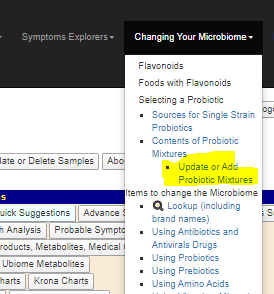
Once you are logged in, a new item appears on the menus as shown below
On the next screen enter a name (including the provider), for example
Or do Thryve/ L. Reu,Rha, being an abbreviated list
Now go back and get your suggestions.. What you just entered will be shown,
Their recommendations is a NEGATIVE in the mixed results, In the Humble Opinion of the Artificial Intelligence behind this page, a poor choice.
Bottom Line
A simple process. If you have your thryve (or other providers) custom probiotic mixtures handy, run them thru add add the results as a comment on this page.
A reader asked me to compile a list of of published studies and articles on the use of antibiotics with ME/CFS. Note that with gut dysbiosis as the model, the choice of antibiotics may depend on the details of the dysbiosis (this a 16s or shotgun GI report is suggested. Xenogene.es offers excellent reports).
At the Whittemore Peterson Institute (WPI) is a non-profit medical research institute dedicated to the support of those with a spectrum of neuro-immune diseases (NIDs) including: myalgic encephalomyelitis, (ME), fibromyalgia, and similar complex chronic diseases of the immune system and the brain. Dr. De Meirleir earned his medical degree from the Vrije Universiteit Brussel in 1977, and completed an internal medicine residency in the Department of Internal Medicine, University Hospital of Vrije Universiteit Brussel. His current research focuses on a subgroup of ME patients who show evidence of chronic bacterial infection and gut dysbiosis. These patients are responding to specific antibiotic/ probiotic therapy.
Chronic Fatigue Syndrome After Q Fever (2007) ” After 4-12 months they developed post-Q-fever fatigue syndrome and were treated with intracellular active antibiotics (fluoroquinolones and tetracycline) for 3-12 months. Efficacy of the treatment was observed in two patients, but in one patient the results were not encouraging. “
Sleep Quality and the Treatment of Intestinal Microbiota Imbalance in Chronic Fatigue Syndrome: A Pilot Study (2015) ” Participants were administered erythromycin 400 mg b.d. for 6 days… Short term antibiotic treatment appears to be insufficient to effect sustainable changes in the gut ecosystem in most CFS participants. Some improvement in objective sleep parameters and mood were found in participants with reduced levels of gram-positive gut microbiota after antibiotic treatment, which is encouraging. Further study of possible links between gut microorganisms and sleep and mood disturbances is warranted. “
Mycoplasma Blood Infection in Chronic Fatigue and Fibromyalgia Syndromes (2003) ” Most patients with CFS/FMS who have mycoplasma infection appear to recover and reach their pre-illness state after long-term antibiotic therapy with doxycycline, and the infection can not be detected after recovery. “
” Dr. Nicolson suggests long-term antibiotic treatment with drugs such as doxycycline, cyprofloxacin, azithromycin, or clarithromycin. By long-term he means a continuous 6-month course of antibiotics followed by multiple 6-week cycles. The extended antibiotic treatment is needed because of “the intracellular locations of mycoplasmas… the slow-growing nature of these infections, their inherent insensitivity to most antibiotics and the persistence of the infections in metabolically inactive forms.” [Src]
Role of Rickettsiae and Chlamydiae in the Psychopathology of Chronic Fatigue Syndrome (CFS) Patients (2000) Results: Group one: 79.5% good and very good results; 4.1% fairly good; 16.4% failed. Group two: 82.3% good and very good results; 2.5% fairly good; 15.2% failed. … All of the Dr. Bottero’s therapeutic results are confirmed since 1991 by Dr. Cecile Jadin of Randburg (South Africa) for more than 3000 CFS and other psychopathological states (300): Sydney 98 CFS Conference, Australia.
A treatment plan (Cecile Jadin’s is similar)
Treatment with antibiotics is difficult because drugs have to penetrate the host cell wall as well as the intracellular organisms. Treatment needs to be prolonged and pulsed, because of continual replication of the intracellular forms. Until adequate diagnostic facilities are readily available treatment needs to be in two stages: the first stage, which is diagnostic, involves the use of two long-term bacteriostatic antibiotics for 6 weeks, and the second, meant to be curative, involves the introduction of a third bactericidal antibiotic.
One possible choice of antibiotics for the first stage is a combination of Doxycycline and Azithromycin. Initially, the Doxycyline needs to be given alone in low dosage for two weeks, because of the risk of a Herxheimer reaction resulting from the release of toxins by damaged bacteria. Such reactions are usually mild and short-lived. If stable after two weeks, Azithromycin in low dosage is added for 4 weeks. Roxithromycin can be used in place of Azithromycin. . Improvement of symptoms, or the occurrence of a Herxheimer reaction, confirms the diagnosis.
Chronic Fatigue Syndrome: A Treatment Guide, Second Edition By Erica Verrillo 2002In this summary by two of the leading researchers
Bottom Line
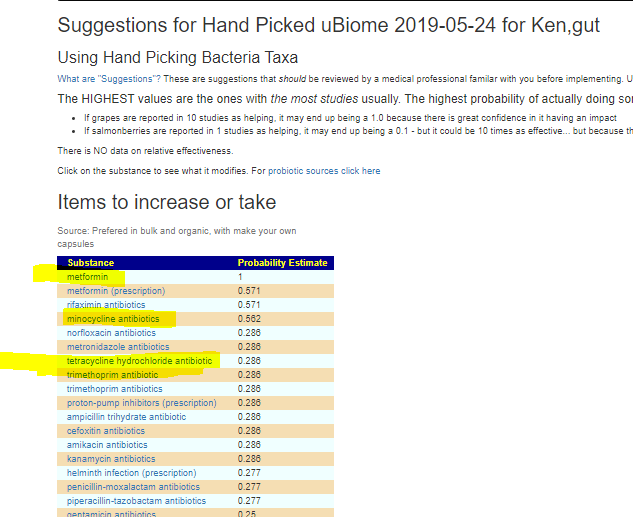
There is a high success rate reported with antibiotics. Recent research suggests that the failures may be selection of inappropriate antibiotics for the person’s specific gut dysbiosis. IMHO, a 16s or shotgun (Xenogene) microbiome report should be done and carefully analyzed prior to selecting the various antibiotics needed.
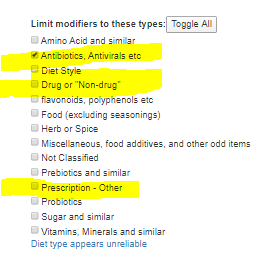
The microbiomePrescription site supports evaluation of antibiotics against a microbiome, as well as other prescription drugs.
Unfortunately, there has been only one comprehensive study done, so relative ranking may not apply for many samples (i.e. do a show all and scan for the ones that are most acceptable)
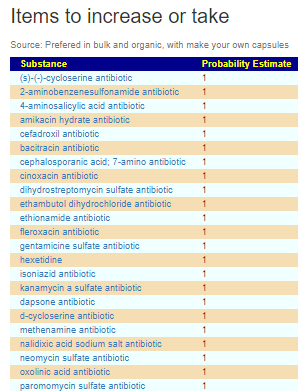
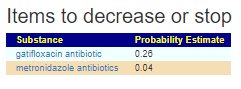
With hand-picking against ME/CFS profiles, results can get quite good. All of the antibiotics involved with prior successful treatment were listed.
A reader wrote me asking about the different theories of ME/CFS, and I just read Cort’s The Best, the Most, the Strangest and the Worst of 2019 in ME/CFS and Fibromyalgia. I have used different models over the years (going with the best available usually). Often it seems that both patients and researchers are lost in the forest strictly following a compass bearing and crossing over paths (and ignoring) that may lead them out of the forest.
My academic training is modelling. A model is a hypothesis with some extra criteria:
Must be predictive
Must be testable
Must explain existing observations
Should be as simple as possible
A good model is one that explains more observations than other models. A good model is one that is easy to test. A good model predicts possible findings (which if the findings comes in correct, confirms the model).
We know that DNA/SNP plays a role – for example, ME/CFS people have smaller hearts, craniocervical instability and certain DNA mutations are more common. These are not causes (people with the same items do not have ME/CFS) but contributing factors that makes people more disposes to developing ME/CFS. Think of the “Perfect Storm”, you have a sea worthy boat — unfortunately you motor died in the middle of gale when you were close to a reef…. a series of unfortunate events.
My criteria for a hypothesis that has merit to investigate or fund — it must give an explanation for the different symptoms! A common response is there are different subsets and we need to identify each subset first, or ‘we have not had time to investigate that yet’ (and likely will never) or even a truthful, “I don’t know” or perhaps a dismissive “that’s not relevant”.
The Microbiome Model explains Symptoms
A rhetoric question — if all of your ME/CFS symptoms disappear do you have ME/CFS. At one time remission was defined as no longer having the minimum number of symptoms required for the CDC definition.
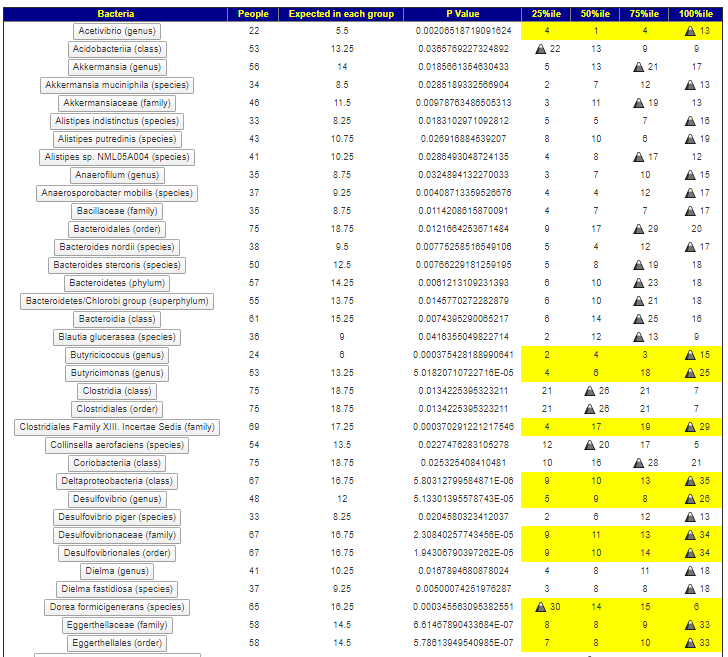
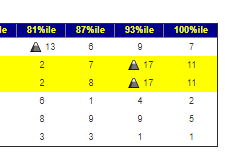
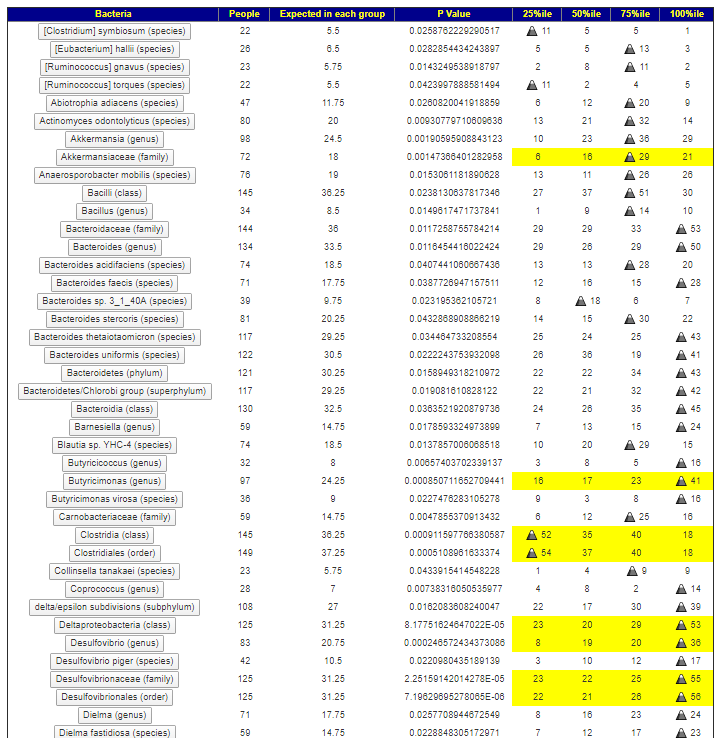
This occurs in a very high percentage of M/E CFS patients. Our analysis found that there were specific microbiome shifts (high levels of certain bacteria)
We find similar patterns, and can drill down to higher resolution (because of more data) and see a strong clustering with people with the highest 15% of some bacteria.
Neurocognitive: Difficulty paying attention for a long period of time
As we walk thru them, we notice overlaps of some bacteria. Look at what is below and alcohol intolerance above. We see the following in common
Butyricimonas (genus)
Deltaproteobacteria (class)
Desulfovibrionales (order)
These are the main players for some ME/CFS, the other bacteria likely cooperate with them to produce specific symptoms (which often have a DNA requirement to appear).
I should point out that a P-value of 0.05 or below is often the criteria for getting a finding published in a medical journal. Some of the values we came up with are 0.000194 and lower. Much much stronger evidence than is usually seen.
Summary
The criteria are below:
Must be predictive
Must be testable
Must explain existing observations
Should be as simple as possible
The microbiome model beats everything else (please add detail comments if you disagree of which model is better using these criteria).
This model is predictive, it can take a microbiome sample in and based on the content alone predict probable symptom (key word is probable) which from my own experience and other user feedback seems around 75% accurate.
This mode is testable, from a microbiome sample we can determine a list of items that would probably help. Some people have had outstanding results. Again, the key word is probable.
This model explain existing observations, the observations we used above in symptoms. Recent research studies also find that it explains many lab results seen with ME/CFS.
This model is simple to understand. It is a beast to work with because of the number of bacteria involved.
The last issues for me are treatment-actionable and available. Most of the research hypothesis do not have treatments to address the cause. A few that do are usually not available — often because it is a research protocol and not “standard of medical care” .. i.e. no one can use, especially the ordinary family physician sitting in a community clinic in the Australian Outback!
The microbiome can be manipulated without prescription drugs which removes the stumbling block of “standard of medical care”. It can even be done under quasi-medical supervision if a patient uses available tools and present the suggestions to their physician for review. Getting physicians up to speed on the microbiome is a different issue.
If you believe a different model is better — then please provide the details in the comments. I am open to changing models.
A reader pointed me to this blog, our2ndbrain.com. He did a DYI FMT transplant using a donation from his daughter [post] and obtained remission.
” For many of you visiting this site, you may have wondered why I picked my daughter as the donor for Fecal Microbiota Transplant. “
Kudos!
I say kudos because this is a very ideal choice of donor! (on the matter of DYI Fmt, I choose, for legal reasons, to keep mute). The whys are simple:
As close to the same DNA as possible (50%)
Same diet (which means that the bacteria mix has already been tuned to the diet)
A son could technically be better (since gender is a factor for the microbiome)
Same longitude (which is a factor)
Younger microbiome — which usually means stronger and more robust. The microbiome “has not slipped into old age”
Bottom Line
I am not advocating people to volunteer to change diapers of their kids and grandkids to get material for DYI FMT. I am advocating, if you have kids (if you do not have kids, if a sibling has children those are better candidates than a random person IMHO), and have a MD willing to go down the FMT path, to advocate for those people as donors, instead of doing the DYI approach on this site.
The following paper gives some background on FMT. There is still disagreement whether family members give better results ( I suspect those studies were done on siblings and not descendents).
[Sattler 1985, Jarisch 2004, Donatelli et al. 1994, Maintz et al. 2006]
Bottom Line
The list are items that you should NOT take because they reduce DAO and can result in fatal histamine reactions if you already have histamine issues. Decision to stop any should be done in consultation with your medical professional.