This is the third of a series of posts dealing with various forms of cognitive impairment that are often age related. My first posts dealt with Alzheimer’s Disease and Parkinson’s Disease. My personal suspicion is that a significant catalyst (if not actual cause) is the lost of microbiome as we age.
The Light Bulb Event
Almost a decade ago, I had a relapse of a condition that I had before and was sent for a SPECT scan. The radiologist suggested that it may be early onset Alzheimer’s. I was having problems with memory then, especially retaining recent memories. In 2017, for the same condition, a patient died and when their brain was examined, this study found
“Among the most remarkable pathological features of the case are focal areas of white matter loss, neurite beading, and neuritic pathology of axons in the white matter with axonal spheroids. Atypical neurons displaying aberrant sprouting processes in response to injury are observed throughout cortical gray and white matter. Abundant amyloid deposits identical to Alzheimer’s disease plaques with accompanying intracellular granular structures are observed as well. Neurofibrillary tangles are also present in the white matter of the frontal cortex, thalamus and basal ganglia. “
For myself, I went into remission. Memory and other issues faded — I am not 100% as strong in some cognitive aspects that I was prior, but to most people they cannot detect the remaining issues.
The condition that I had was successfully treated using a protocol that altered the microbiome. What if this was true for other similar conditions — especially the untreatable ones? Recent literature appears to support this.
- “More recently, microbial dysbiosis has been associated with a number of brain pathologies, including autism spectrum disorder, Alzheimer’s disease (AD), Parkinson’s disease (PD), and amyotrophic lateral sclerosis (ALS), suggesting a direct or indirect communication between intestinal bacteria and the central nervous system (CNS). ” [2018]
- “Recent data suggest that dysbiosis of gut microbiota may contribute to ALS etiology and progression. ” [2018]
- “Here we present evidence that intestinal dysfunction and dysbiosis may actively contribute to ALS pathophysiology.” [2017]
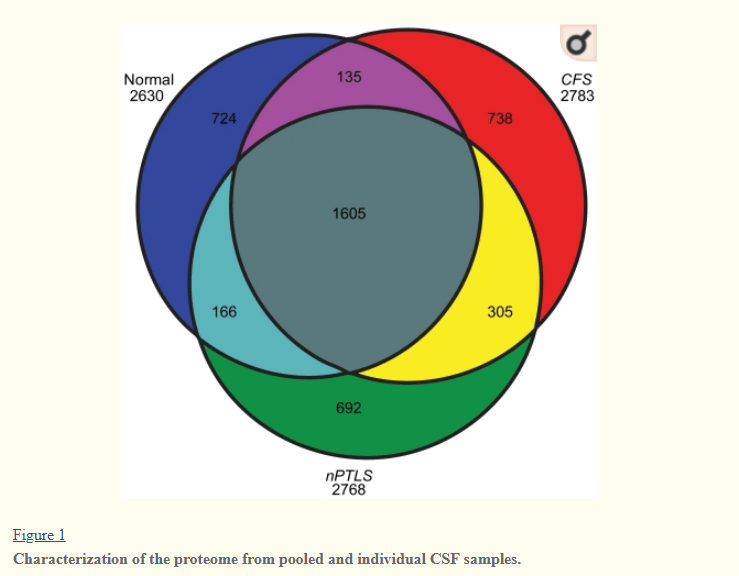
CSF Proteins Dimension
A 2011 Study found that Cerebrospinal Fluid Proteomes were different for my condition, a normal population and PTSD. These CFP’s are also heavily studied with ALS ( 2015 Study) ” Ten proteins were differently regulated in ALS CSF compared to controls in at least 2 studies. ” [2017] – both have novel proteins (i.e. proteins not seen in a healthy population). “We identified significant differences in the CSF proteomebetween living and post mortem ALS subjects, as well as living and post mortem control subjects. We also noted differences in the CSF proteome of ALS subjects that have exhibited symptoms for varying lengths of time and between ALS and Alzheimer’s Disease subjects at end-stage of disease.” [2007]
Working Hypothesis
My working hypothesis is that these CSF proteins are due to microbiome disruption. This disruption may not be a magic bacteria that causes it, but due to undersupply or oversupply of metabolites causing epigenetic changes in the bacteria resulting in these new proteins. Unlike both Parkinson’s Disease and Alzheimer’s disease, I could not find any studies of ALS and Bacteroides fragilis with humans. But with ALS mice (G93A), we see that in studies.
- “When stressed, overpopulated or pathogenically stimulated, B. fragilis releases a remarkably complex array of endotoxins and exotoxins (such as fagilysin), lipooligosaccahrides (LOS), lipopolysaccharide (LPS), including an extremely proinflammatory B. fragilis LPS (BF-LPS), microRNA-like sncRNA, and a wide variety of bacterial-derived amyloids (9–11, 56, 57, 64–66). ” [2018]
You may wish to read my Reducing bacteroides fragilis
Hypothesis Tests
The hypothesis implies that there would distinctive shifts in bacteria seen with AD. What does the literature say?
- “In a small study of ALS patients and healthy controls, investigators also found decreased levels of butyrate-producing bacteria. ” [2018]
- “The comparison between ALS subjects and healthy group revealed a variation in the intestinal microbial composition with a higher abundance of E. coli and enterobacteria and a low abundance of total yeast in patients. ” [2018]
- “In mice fed with butyrate, intestinal microbial homeostasis was restored, gut integrity was improved, and life span was prolonged compared with those in control mice.” [2017]
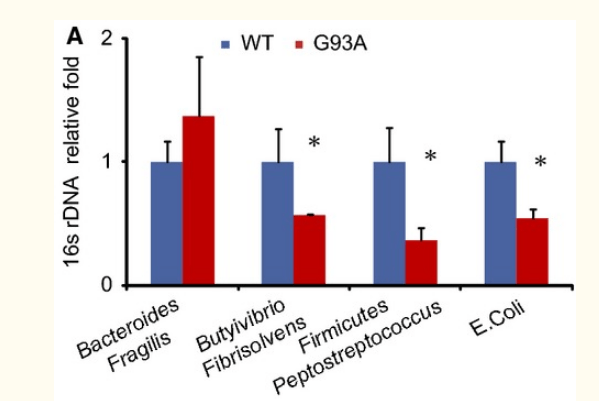
- “These changes were associated with a shifted profile of the intestinal microbiome, including reduced levels of Butyrivibrio Fibrisolvens, Escherichia coli, and Fermicus, in G93A mice. The relative abundance of bacteria was shifted in G93A mice compared to wild-type mice. Principal coordinate analysis indicated a difference in fecal microbial communities between ALS and wild-type mice. ” [2015]
- “the top 10 microorganism populations were analyzed at genus level, and average ratios f Bacteroides, Faecalibacterium, Anaerostipes, Prevotella, Escherichia, and Lachnospira between groups A and H were 0.78, 2.18, 3.41, 0.35, 0.79, and 13.07 (Figure Figure33). Furthermore, supervised comparisons by LEfSE (LDA > 4.0) were performed to find the significant changed bacteria, and the relative richness of Firmicutes at phylum level, Clostridia at class level, Clostridiales at order level, Lachnospiraceae and Family XIII at family level, Oscillibacter, Anaerostipes and Lachnospiraceae at genus level in group H were significant higher than that in group A, while Bacteroidetes at phylum level, Bacteroidia at class level, Bacteroidales at order level and Dorea at genus level were significant higher in group A” H:Health A: ALS [2016]
- “The present study suggested that higher intake of fat and protein, particularly from meat at early stage of the disease, could prolong the survival of ALS patients. ” [2018] This modifies the microbiome, see this summary.
- “A large portion of patients with ALS exhibited poor dietary intake and changes in body zinc status. The zinc deficiency found in half of the ALS patients may contribute to a worsened prognosis and should be the target of nutritional intervention that aims to correct this deficiency.” [2017] This modifies the microbiome, see this summary
- Association Between Dietary Intake and Function in Amyotrophic Lateral Sclerosis. [2016]
- ” In replicated experiments, we found that chronic dietary exposure to a cyanobacterial toxin present in the traditional Chamorro diet, β-N-methylamino-l-alanine (BMAA), triggers the formation of both NFT and β-amyloid deposits similar in structure and density to those found in brain tissues of Chamorros who died with ALS/PDC. Vervets (Chlorocebus sabaeus) fed for 140 days with BMAA-dosed fruit developed NFT and sparse β-amyloid deposits in the brain. Co-administration of the dietary amino acid l-serine with l-BMAA significantly reduced the density of NFT.” [2016] l-serine modifies gut bacteria.
Bottom Line
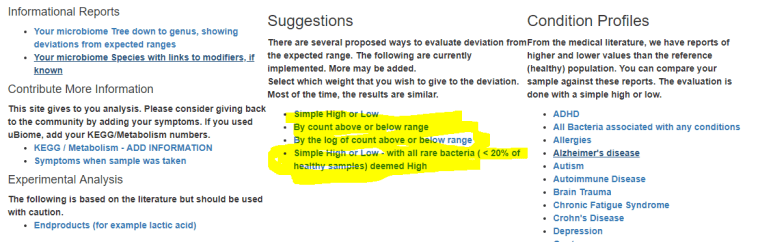
If you are a carer for someone with amyotrophic lateral sclerosis, you may wish to get a 16S analysis done ( for example uBiome.com – < $100) and upload the results to http://microbiomeprescription.com/. The suggestions there are based on hundreds of studies of what shifts different members of the microbiome. It’s a free site and the information is not available easily any wherelse.
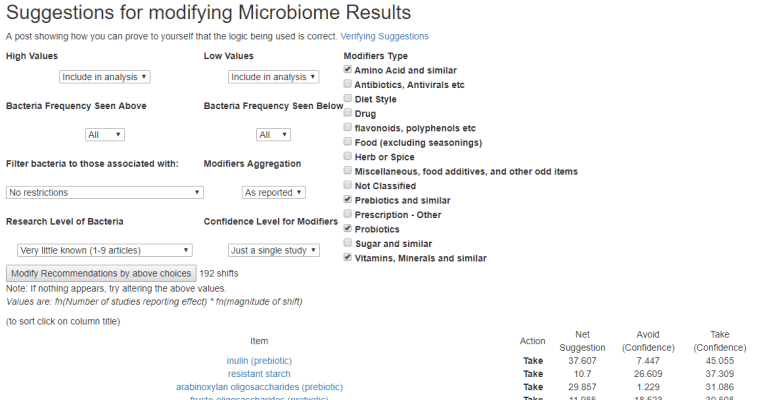
An example of getting suggestions is shown in this post.
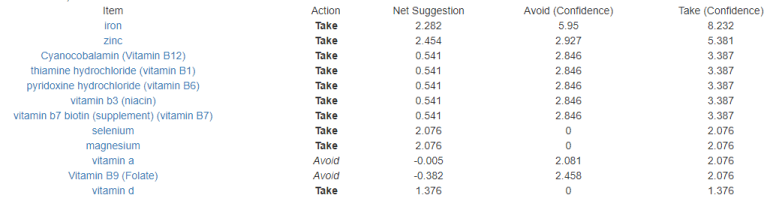
I have updated the ALS Microbiome template on that site, i.e.
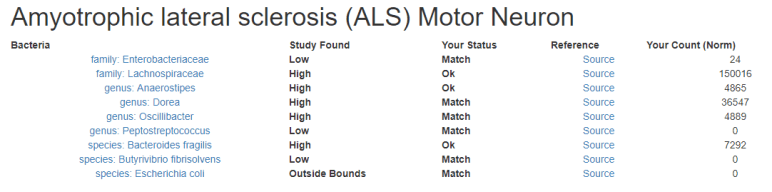
Look at the suggestions and discuss them with your treating physician.
This is an education post to facilitate discussing this approach with your medical professionals. It is not medical advice for the treatment of any medical condition. Always consult with your medical professional before doing any changes of diet, supplements or activity. Some items cites may interfere with prescription medicines.