
Ran into some issues using “ubiome” in the website name address.
Site is now:
http://microbiomeprescription.com/
I had to roll back to an older version of the site — because I was in the midst of an enhancement.
No data has been lost.
Ran into some issues using “ubiome” in the website name address.
Site is now:
http://microbiomeprescription.com/
I had to roll back to an older version of the site — because I was in the midst of an enhancement.
No data has been lost.
This weekend I hope to finish making changes so that throat, nose and other ubiome samples may also be investigated.
Symptoms will be linked to the email + sample date, so there is no need to re-enter symptoms. This would allow people to see the impact of changes in mouth health by changes in habits they implemented.
Recommendations will continue to be ONLY for gut — there are not enough studies to venture into other areas. BUT, if you start chewing mastic gum (something that I have suggested before), you should see the impact on your throat and nose bacteria.
Many items appear under 3-6 different names in the literature. The citation used the term used in the study. The simplification will replace things like:
with just resveratrol (whatever the common name of a supplement is).
This will impact some recommendations because we will stop double counting or under counting some modifiers.
In my earlier post, COMPARING REPEATED UBIOME RESULTS, I provided a tool but little guidance on interpreting. The key question is always whether the symptoms improved, not whether some numbers change. We do not know which numbers are significant and which numbers are just natural variation.
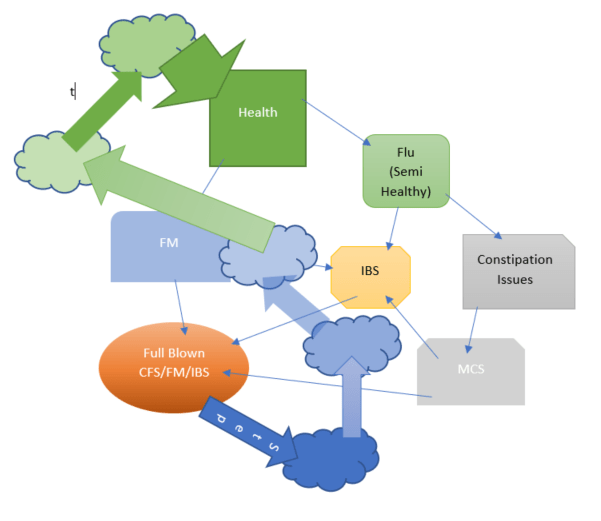
People see progression of symptoms since onset. Each progression is likely associated with a set of changes in the uBiome. This can be represented in the chart below (which likely have a lot more items than shown).

This appears to happen in two scenarios:
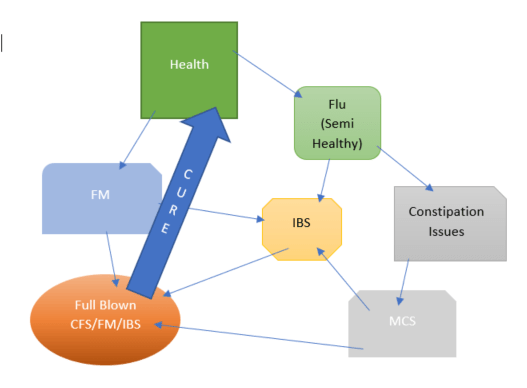
This model comes from the model that we may have more than a dozen bacteria groups involved in the symptoms. For depression alone, we see 28!!. Being able to correct all of them in one-go is not likely. You may correct one and those not effected adapt to try entrenching themselves better (like filling the empty space of the bacteria reduced).
I am looking at a person with two samples. I have not automated the comparisons shown below, instead I selected a sample and then went to the page and did a simple count.
Over all, we went from 31 matches to 27 matches. One increased and three decreased — I wish it was possible to do decrease across all items…
The original detail was done as a quickly and dirty report comparing numbers and attempts to keep people from becoming excessively focus on numbers (which we are not certain of significance – some are likely important and some are not… we do not know for sure which ones are).
From feedback, it is clear that a simpler report, the summary, would be easier to understand and likely more beneficial
Time between samples: 10 months
Like the profiles used above, this filters ‘noise’ and looks at the net result of a lot of different bacteria. I have just added a new item to the report
Average Metabolism (Ideal healthy would be 1.0)
In short, the metabolism is improving greatly.
There are now two buttons available for comparison

The new report is Summary, and an example is shown below. The most significant ones are high lighted.
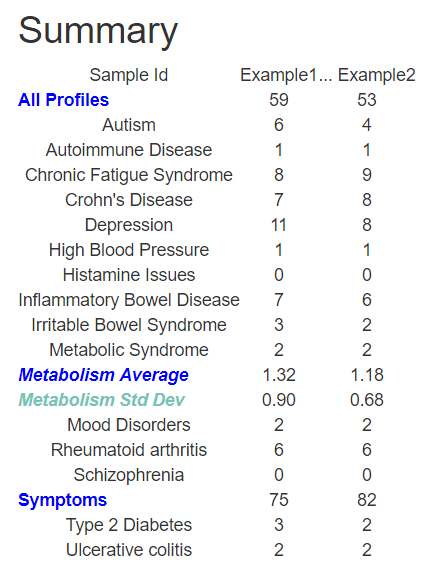
The new summary page give you three objective measures of your progress. For the reader above, all three objective measures improved. The subjective measure (number of symptoms) increased — we do not record severity of symptoms because that is so-so-so very subjective, just a count.
The reader found that the recommendations changed a lot between the two samples. A change is expected if progress is made. Conceptually, the number of items with a high (or low — for avoid) should decrease if progress is made. We see this in the samples of this reader, as shown below.
For Example 1, we had the > 4 take
amoxicillin
Azithromycin
florfenicol
Cranberry bean flour
Bacillus subtilis natto
Gallate
Flaxseed
High Fat
Plant-rich diet
ß-lactam antibiotics
Tannin
Trimethoprim-sulfamethoxazole
Vitamin D
Polymannuronic acid
For Example 2, the list has grown smaller, with some new items appearing
Polymannuronic acid
Ketogenic diet
Lactobacillus kefiri
Low fat diets
L-Taurine
Lactobacillus plantarum
Bacillus subtilis natto
For Exampl1, the < -4 list
Arabinoxylans
black raspberries
Acetic acid
Chrysanthemum morifolium
ibuprofen
Isobutyric acid
Isovaleric acid
Sunflower Oil
High fruit intake
barley
Saccharin
Saccharomyces boulardii
animal-based protein
High meat diet
Fraxinus angustifolia
berberine
For Example 2, the list is again smaller for < -4, with a few items in common
Walnuts
Navy bean
berberine
High protein diet
Carboxymethyl cellulose
Polysorbate 80
ku ding cha tea
barley
Fraxinus angustifolia
I have done a few posts on depression over the years
A friend asked me to revisit it, especially now that I have a recommendation program working.
Altered fecal microbiota composition in patients with major depressive disorder [2015]. adds that “Bacterial diversity was significantly higher ” and also reported additionally (for two types of depression):
Additionally, Isovaleric acid in stool correlates with human depression.[2016] hence isovaleric acid producing bacteria appear to be another facet.
Isovaleric acid producing bacteria includes [ref]:
After you logged on to http://microbiomeprescription.com/ This Depression link will show your results against the above list. As a reminder, there are other comparisons available:
The result is a report such as shown below

At the bottom is a link to recommendations for the ‘Match’ items above only. That is, the recommendations are specific to the depression symptom.

For the first one on the list, I did a google and found lots of pages saying that pomegranate helps depression!
Imagine that! With the microbiome approach, you are getting truly individualized suggestions and not proforma suggestions.
This is an education post to facilitate discussing this approach with your medical professionals. It is not medical advice for the treatment of any medical condition. Always consult with your medical professional before doing any changes of diet, supplements or activity. Some items cites may interfere with prescription medicines.
A reader sent these questions to me
An Interview with Ken Lassesen
| Much Better | Better | no change | Worst | Much Word | Herx Stopped | Odds Ratio | |
| minocycline | 2 | 3 | 1 | 2 | 2 | 0 | 125% |
| rifampicin | 0 | 0 | 0 | 2 | 0 | 0 | 0% |
| doxycycline | 5 | 5 | 2 | 3 | 1 | 1 | 200% |
| Azithromycin | 4 | 9 | 2 | 1 | 2 | 0 | 433% |
| Ciprofloxacin | 0 | 3 | 1 | 0 | 2 | 2 | 75% |
| Metronidazole | 0 | 5 | 4 | 0 | 1 | 0 | 500% |
| Amoxicillian | 0 | 4 | 2 | 5 | 2 | 2 | 44% |
| Bacitracin | 0 | 2 | 0 | 0 | 0 | 0 | |
| Sulfacetamine | 0 | 1 | 0 | 3 | 0 | 1 | 25% |
| Tinidazole | 1 | 4 | 1 | 1 | 0 | 0 | 500% |
