
This is from a reader that I have been corresponding with since 2017 and known from online groups for decades..
Okay, you don’t want the full saga 😀 (joking ) and so I’ll write the first current impressions of a ME/CFS patient since 1998. I am someone who has tried everything; really everything.
First of all, as I had already told you in chat, I use as a criterion of improvement in the disease the increase in cardiovascular tone, which actually happened for a short time as long as I kept a diet that was not exactly ironclad, but very difficult for me: it involved cutting out all refined sugars.For those interested, I talked about it here : https://www.fable.it/fluorochinoloni-hrv-dieta-e-me-cfs/ (in Italian — use Google translate) . For the first seven days of the diet nothing changed, nothing! After these 7 days suddenly, keeping to this diet , cardiovascular tone started to increase until … well … I kept the rest of the diet but reintroduced sugars (but not alcohol). Then improvement stopped (but maintained existing improvements).
From Reader
Recent significant events are:
- fluoroquinolones toxicity in 2020
- supplements of akkermansia muciniphila one month before last sample (see below for his experience)
Ancient Test Results
A test result from 23 August 2016 is below. The test show only few bacteria without any ranges of normal valid. We will compare the few items reported with the latest Biomesight test. There was little change over 7 years.
Any persistent Fluoroquinolones artifacts?
I did a behind the UI Meanings? Comparison of what Fluoroquinolones changed with his sample. Although it has been 3 years, I am curious. No impact would have 50-50 agreement. In the result? We have 64 bacteria showing the effect that that Fluoroquinolones would cause, and 43 showing the opposite effect. This results in a P-Value of 0.0423 from chi-square. A P-value below 0.05 is deemed statistically significant in medical studies. So, this is evidence that the impact of Fluoroquinolones is still there after 3 years.
This is an interesting observation — picking the wrong antibiotic may have effects that persists for years.
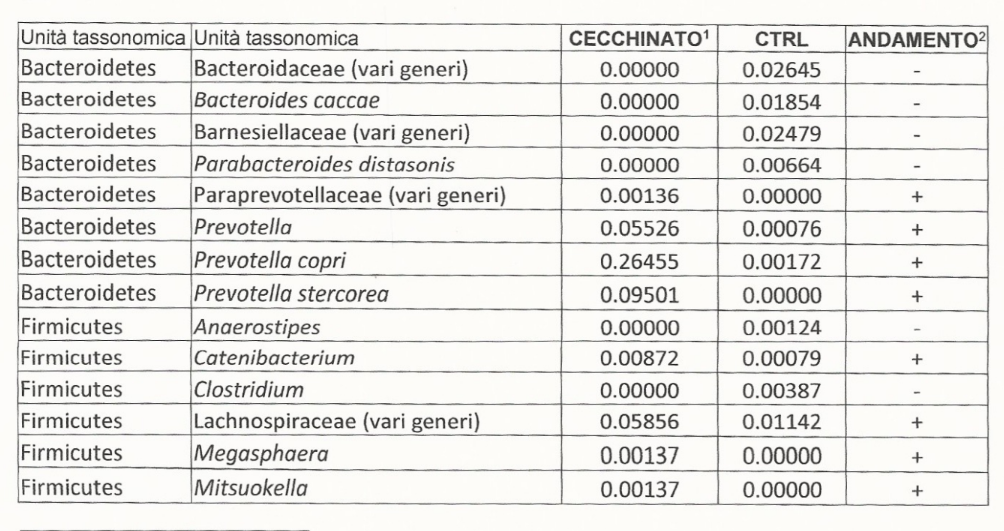
Comparing to Ancient Test Shown Above
Each lab uses their own methodologies to measurements (See The taxonomy nightmare before Christmas… for why and Comparing Microbiomes from Three Different Providers for actual example). So we cannot determine if the levels have gone up or down.
- Bacteroides caccae is at 15%ile, still low
- Barnesiellaceae is 0%ile, still low
- Parabacteroides distasonis is 12%ile, still low
- Prevotellaceae is 97%ile, still high
- Prevotella is 97%ile, still high
- Prevotella copri is 95%ile, still high
- Prevotella stercorea is 96%ile, still high
- Anaerostipes is 0%ile, still low
- Catenibacterium is 93%ile, still high
- Clostridium is 26%ile, still low
- Lachnospiraceae is 2%ile, was high
- Megasphaera is 95%ile, still high
- Mitsuokella was not reported, was high
The microbiome was been relatively stable over 7 years. In fact, the Biomesight test clarify how extreme the values are (which is not clear from the earlier report).
Where do we go from here?
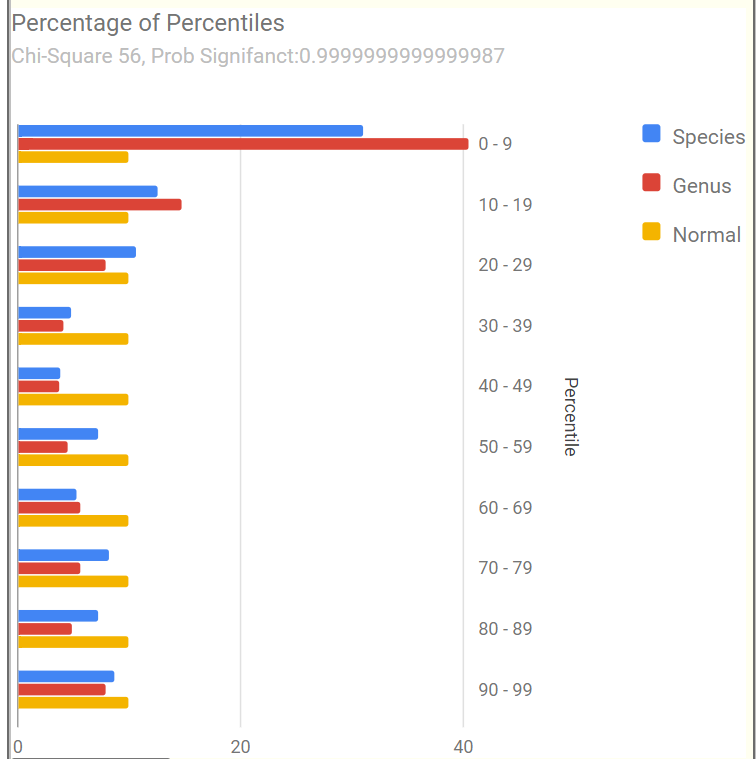
The Percentage of Percentiles pattern shown below is a match for that seen with many ME/CFS or Long COVID microbiome.
Nerdy Explanation: Using percentiles, the data is transformed to an uniform distribution. An unbiased sample (a.k.a. normal or healthy), would have the same number in each 10%ile range. It does not. We have the typical spike in the 0-9%ile range (i.e. too many species and genus that have token representation).
The most important/concerning bacteria identified was Prevotella copri. This bacteria made up 43% of the microbiome!!!! This bacteria is often associated with mycotoxin being present in the environment [2020]. In simple words, Prevotella increases when there is mold in the environment, the chemicals that the mold gives off, feed this bacteria. This usually means examining the living space for mold and fungi, as well as avoiding foods likely to have mold (see WHO for more information). His response to this comment was:
Yes, I live in a north-oriented flat where there is never sun on the walls. Only in a bedroom not used anymore as bedroom I have visible mold (picture attached). I have tried treating with chlorine bleach. In February 2023, I called in a painter. He treated with anti mold solution and thermal painting (which can be dangerous. I wouldn’t lived in that bedroom till the smell went away.
From Reader
And yes, being in the sun recharge me. I don’t know if it also affects mycotoxins. However in my block / area where I live, we never have less than 60% humidity, but in summer usually we have 70-75% so… humidity is a concern.
There are many sites providing suggestions on this issue, a few are: [Aircare Hawaii] and this
Is mold related to humidity?
European and Italian homes are typically built with reinforced concrete frames and brick walls.
Walls and ceiling surfaces are finished with mortar/plaster and water base paint. As water base
paint is not waterproof, plaster finishing tends to absorb and retain humidity. These areas can
become damp or wet as a result of a water leak or condensation of vapors produced by appliances
and normal household activities.
The use of a waterproof paint after cleaning (and running a dehumidifier) in the bedroom is one possible approach. Reader responded (to his delight) that water proof paint was used!
Mold and ME/CFS Relationship
“Urine specimens from 104 of 112 patients (93%) were positive for at least one mycotoxin” from Detection of Mycotoxins in Patients with Chronic Fatigue Syndrome [2013]
“Environmental factors – exposure to mold or toxins has been suspected as a trigger for ME/CFS. However, associations of specific environmental factors with ME/CFS have not been established.” [CDC]
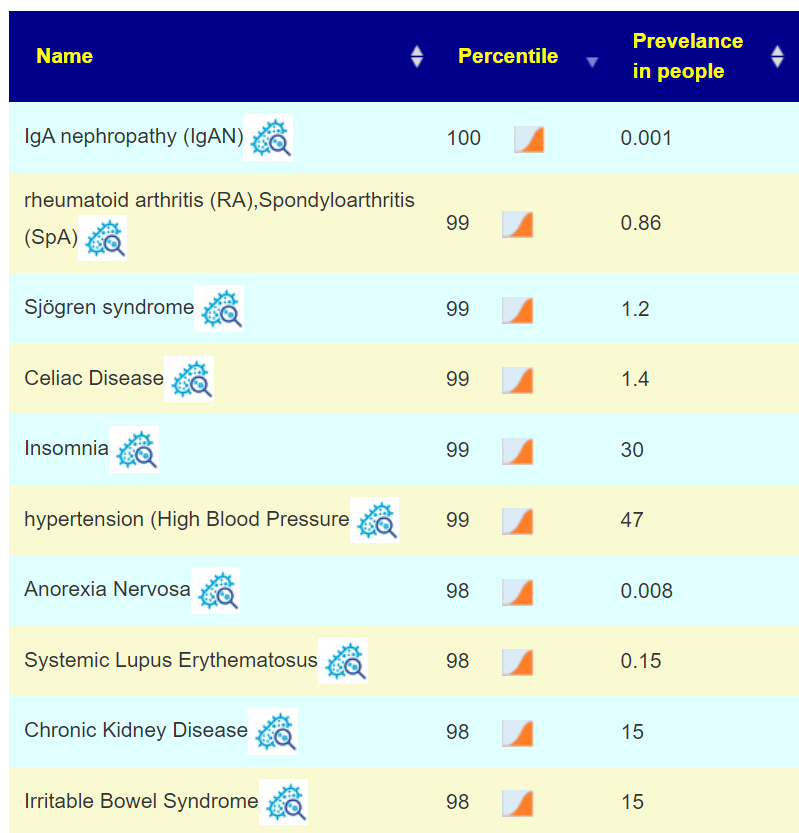
This plus other shifts, matches to a host of conditions shown below. Many are co-morbid with ME/CFS.
The Computed Probiotics from KEGG Enzymes had some very high numbers (over 600!). High numbers mean that there count of many enzymes being produced by your microbiome is very low. This is important because processing of food may be disrupted. Some of these are available in probiotics, with the top feasible suggestions being:
- Escherichia coli
- Brevibacillus brevis
- Bacillus subtilis
- Bacillus licheniformis
- Bacillus subtilis subsp. natto
- Clostridium butyricum
Two retail probiotics for the Bacillus above are: Energybalance / ColoBiotica 28 Colon Support and microbiome labs/ megasporebiotic. The person is in Europe, so the two E.Coli probiotics: Symbioflor-2 and Mutaflor are available. For others, see Probiotic Mixtures.
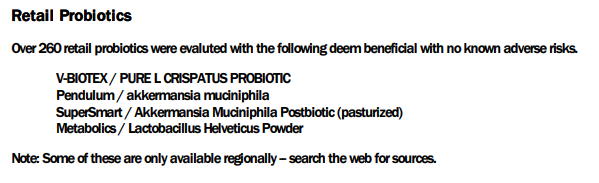
I will defer the rest of the suggestions to the PDF, attached below. It is interesting to note that akkermansia muciniphila probiotics is well recommended (see experience below).
In this case, we have good positive reader experience happening before the suggestion was made! It should encourage the reader to trust the other suggestions (after all, “one suggestion worked before he got it!” 🙂 )
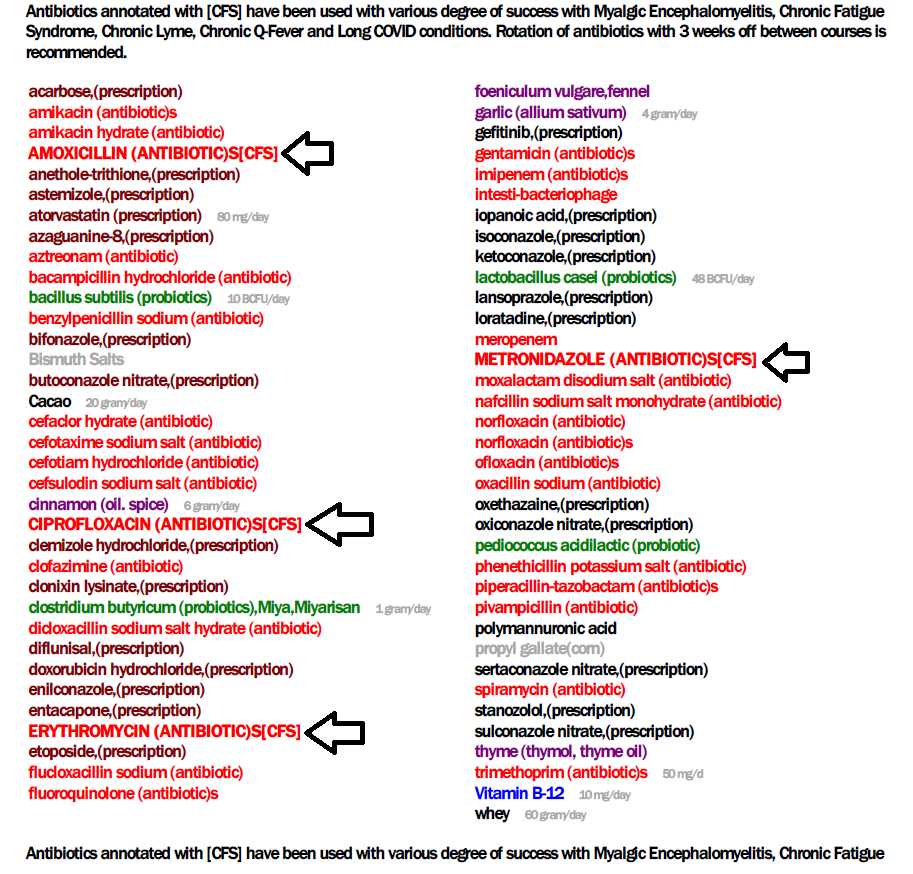
I also looked at the MD version which suggested a few antibiotics:
- oxytetracycline dihydrate (antibiotic) – a broad-spectrum tetracycline antibiotic
- thiamphenicol (antibiotic)
- ß-lactam (antibiotic)s (33% of p.copri resistant [2022])
None of these are typically used for ME/CFS (but other tetracyclines are). We have one big target: P.Copri. I am hoping that you have a cooperative MD. I checked around for information on antibiotics which often have little effect on P.Copri, these studies have extensive lists.
- Antibiotic resistance in Prevotella species isolated from patients with cystic fibrosis [2013] – you want runs with R being a zero (0) in Table 1
- I am inclined to metronidazole, which is often used in treating ME/CFS (also in this 2010 study), and 98% effectiveness reported in this 2019 study.
- I am inclined to metronidazole, which is often used in treating ME/CFS (also in this 2010 study), and 98% effectiveness reported in this 2019 study.
Akkermansia Muciniphila Experience
Another thing Ken, is the sensational discovery this year of Akkermnasia Probiotics (in my case from Metagenics). In my first two days I went from going to the bathroom once a day to going three four times. How many times have we read that a normal bowel transit involves 1 evacuation a day to one every 2-3 days ? No ! The ideal transit is to go to the bathroom about half an hour after eating ! Well, this happened to me while supplementing Akkermansia once a day. And it is only one strain !!! Not only that ! I felt less “Fight or Flight” but more serene, even when I woke up from my night sleep. Even with scabs on my eyes that who knows how many years I haven’t found (how many of us have perpetually dry eyes ?). I stopped the supplementation after a month and am now resuming it.
From Reader
Why am I writing you this Ken ? To waste your time !!! No, I am writing this to you because I had first read about this Akkermansia three years ago on the label of an Austrian product, Omni Logic Plus, which contains a lot of good stuff (FOS, GOS , etc.) to feed this specific bacteria, Akkermansia . Three years of supplementation every day has not improved anything.
After just a few days of Akkermansia , that is, the strain that that Omni Logic Plus was supposed to feed, did the miracle happen! What do I mean by all this ? That , my thought is that rather than depending on the food, if they are available as supplements, little bacterial strains should be introduced, for a far better effect.
Questions:
Q: When the “nutrients” of the supernumerary bacteria are present they grow. If you cut off their nutrients, the effect on microbiota diversity is extremely “reactive” !!! Did this happen when I removed the sugars ?? Do you agree with my reasoning ?
- A: Yes — consider a human population that is well fed (obese even). If you suddenly impose strict rationing on them, their behavior changes greatly (often with criminal actions).
Q: Is it more effective to remove the food that feeds the overrepresented bacteria and simultaneously supplement the underrepresented strains not so much with diet and food, but with probiotics ?
An example of my personal case ? When in the report generated by your site I see among the recommendations clostridium butyricum , which I’ve never tried in my life.
- A: The algorithms effectively does that — identifies suggestions reduced high bacteria while checking that it does not further reduce low bacteria of concern. Also the reverse, suggestions increases low bacteria while checking that it does not further increase high bacteria of concern.. You can try to calculate these manually — but its a massive amount of reading and searching. Microbiome Prescription uses some 1.8 million facts pulled from almost 12,000 studies.
Q: Who knows if it can give me the same benefits as Akkermansia? After years where for weeks on end , I have tried various products. Like everyone else, I have been spending hundreds of Euros. For example:
- probactiol duo ( billions of Saccharomyces boulardii)
- 8.5 billion of a probiotic blend – HOWARU blend (Lactobacillus acidophilus NCFM®, Bifidobacterium lactis Bi-07®, Lactobacillus paracasei Lpc37™, Bifidobacterium lactis Bi-04™)
- A: The purpose of Microbiome Prescription is to compute the most likely ones based on your microbiome and what studies reports the effects of various probiotics are. This means greatly increased odds of positive effects! Much better (and cheaper in the long run) than trying things suggested by influencers or which worked for someone with a very different microbiome.
Your list is very short — 50% is what you recently discovered works!!
For probiotics, do one at a time for 10 days then rotate to another. Why? Their effect is often due to natural antibiotics that they produce. Keeping on them continuously allows “natural antibiotic resistance” to develop.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide solid information on rotations, dosages, etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting. Some suggestions may be counterindicated for other medications you are taking and medical conditions.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.


{kind=link}