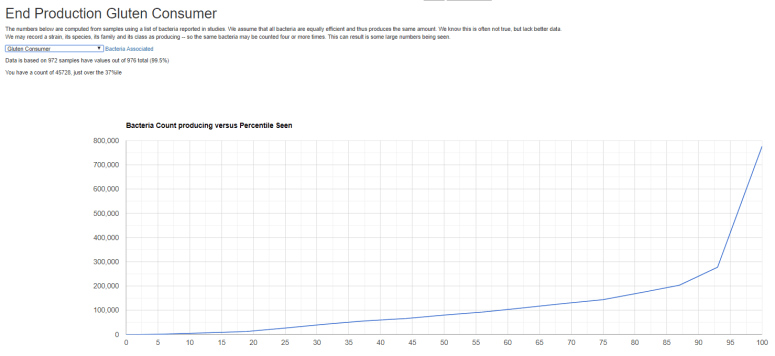
I have a regular task of manual reviewing potential studies selected by Textural Analysis (Artificial Intelligence/Data Science) published on PubMed. The count of articles reviewed by the AI and myself (for those that the AI selected) is up to 456,847 with many more to go. One of these articles listed the bacteria identified by this study (from human samples) that consumes/process gluten.
It is logical to hypothesis that gluten intolerance/issues is connected to the absence/low numbers of these bacterias.
A reader asks me to do a recap of what the known shifts are, and thus what you wish to try to correct (and not inadvertently increase by the wrong supplements, probiotics or diet choices).
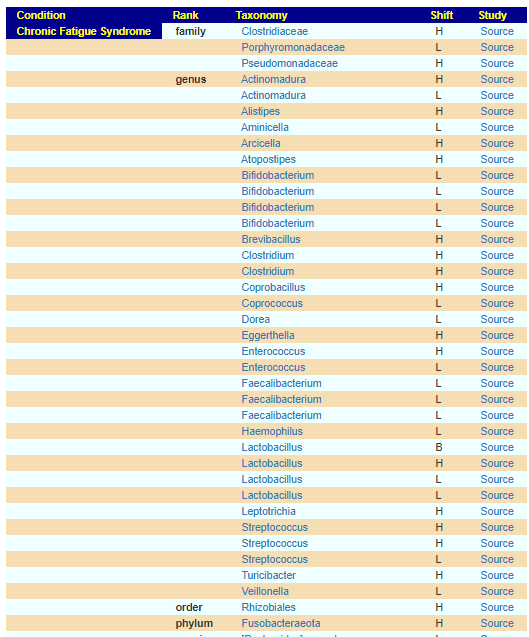
In terms of published studies, I have assembled a dynamic list on my website (not verified and subject to data entry errors) shown below for genus level and above. When an item is repeated on multiple lines, this means that we have multiple studies report it. H-High, L- Low, B- High or Low (outside of normal)
It is unlikely that every ME/CFS will have all of these shifts. Most will have some.
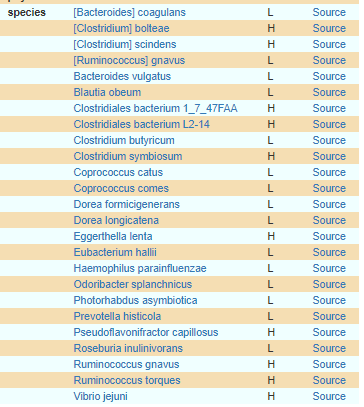
At the Strain Level, we also have a long list,
Remember, for Low, it is not uncommon for people to have none of these and be perfectly healthy. The Low count is from the average of the group in the study and not definitive for any individual.
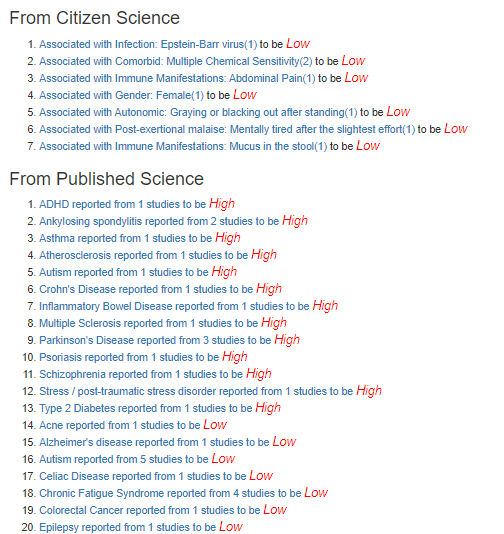
Using the citizen science aspect of my site, we do not have a information based on physician verification of precise clinical definition but solely on self-reporting of symptoms. If click on one of the above, say Bifidobacterium, we see two things listed:
Citizen Science discoveries dealing with symptoms.
Published studies listing conditions that may have the same shift (thus, potential conditions that ME/CFS may evolve to).
For 1 (EBV),2 (MCS), 4(Female), 5, 6 (Post exertional malaise) are in the list of items that are used for a ME/CFS diagnosis
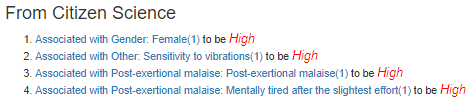
Going over to Faecalibacterium (3 citations) – another LOW one, we see a more massive symptom list, many many are in the classic ME/CFS diagnosis list.
Doing another one, Streptococcus – a HIGH one for a change (3 citations – 2 high and 1 low), we see
Double Validation
One list of bacteria comes from studies on patients that conform to strict definitions of ME/CFS. The other list of bacteria comes out of the symptoms people self-report and their 16s microbiome results. We have a very strong agreement with the results coming from two independent approaches.
What does this mean?
It means that altering the microbiome will improve symptoms (as indicated in the study cited at the start; and in personal agreement with my own experience and many of my readers).
The next step is to determine which of these long lists of bacteria is involved with your ME/CFS/IBS etc. The old conventional tests only does a few of the bacteria — and do not cover all of those reported in studies. By old conventional tests, I mean:
Once you know the bacteria involved, you need to know how to change them. If your physician, nutritionist or other health professional are well skilled and read on the microbiome, they should be able to guide you.
If they are not, I have created my free analysis and suggestion artificial intelligence engine http://microbiomeprescription.com/ which uses over 95,000 medical facts on the microbiome. You must review those suggestions with your medical profession because some may be inappropriate given other medical conditions.
The Candida species play a role in a healthy body. It is when there is too many that problems start. A friend asked me to put together what we know based on published studies only, no urban-medical-beliefs.
There is an increased total fungal load particularly of Candida and Malassezia species in the faeces and mucosa of Crohn’s disease patients, and a lower fungal diversity in the faeces of ulcerative colitis patients. [2019]
These are cited, with further studies on this page (in french) and includes the above with links to multiple additional studies for each.
Other Stuff
” It can be concluded that monolaurin has a potential antifungal activity against C. albicans and can modulate the pro-inflammatory response of the host. ” [2016]
” The difference between the groups [chlorhexidine, lactobacillus probiotics, coconut oil] was not statistically significant (Chi-square value 7.42, P value 0.06). ” [2016]
” Eucommia ulmoides, Polygonum cuspidatum, Poria cocos and Uncaria rhyncophylla showed activity against both bacterial and fungal strains, indicating their broad spectrum of activity. ” [2013]
” Data show that mustard [i.e. Turmeric] and coconut oil seem to be effective as in these the spore germination was poor. ” 1992
Pau D’Arco ( Tabebuia ) – Studies found no significant effect [1994]
“Tabebuia avellanedae (methanol extract), with MIC varying from 0.06 to 0.001 mg/mL; ” [2010] – this is a fraction of the effectiveness of items above.
Probiotics
Enterococcus Faecalis appears effective [2014] (available as probiotic)
Lactobacillus GG, Lactobacillus rhamnosus LC705 and Propionibacterium freudenreichii ssp. shermanii JS was shown to be an effective means of controlling oral Candida and hypo‐salivation in the elderly (Hatakka et al. 2007). [2016]
Bacillus subtilis exhibited clear zones of inhibition for Candida albicans and Candida parapsilosis but not for Candida krusei. [2016]
Sookkhee et al., in 2001, studied the effects on Candida albicans growth of different lactic-acid bacteria isolated from the oral cavity of volunteers and found that two strains, Lactobacillus paracasei and Lactobacillus rhamnosus, had the strongest effect on the yeast [44]. Lactobacillus reuteriis a promising bacterium (especially DSM 17938 and ATCC PTA 5289) for its anti-Candida properties, confirmed by several studies. In one of these, Lactobacillus reuteri was demonstrated to be able to reduce Candida load in vivo through co-aggregation, modification of oral pH with production of lactic acid and other organic acids that inhibit the virulence of Candida cells, and production of H2O2 [45]. In a recent in vitro study by Coman et al. (2014), the strains Lactobacillus rhamnosus IMC 501 and lactobacillus paracasei IMC 502, alone or in combination, showed an inhibitory effect on Candida spp. growth [46]. Lactobacillus delbrueckii ssp. bulgaricus B1 and Lactobacillus delbrueckii ssp. bulgaricus TAB2 were found to fight Candida, releasing high amounts of lactic acid [47].Recently, it was found that Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14 modulate Candida glabrata virulence, through the complete inhibition of fungal biofilms [48].In addition, Lactobacillus acidophilus ATCC 4356 was found to inhibit the biofilm formation of fungus through in vitro experiments [49]. Biofilm formation is probably reduced through the production of substances called “bacteriocins” by probiotics. Wannun et al. reported the isolation of a bacteriocin, called “fermencin SD11”, from Lactobacillus fermentumSD11, a human oral Lactobacillus, which has a strong inhibitory effect on oral Candida cells [50].
Effect of Probiotics on Oral Candidiasis: A Systematic Review and Meta-Analysis 2019
Histamine Caution
All Lactobacillus Reuteri are histamine producers.
Many Bacillus subtilis are histamine producers [2007]
Lactobacillus rhamnosus appears not to be a histamine producer and reduces histamines [2011]
Or, all gluten is not the same — just like all cheese are not the same. People may have issues with one type of gluten — especially wheat gluten where there was been many generations of genetic manipulations to produce more profitable wheat harvests.
This is of concern to me in dealing with people with microbiome dysfunction – such as Myalgic encephalomyelitis/chronic fatigue syndrome and even fibromyalgia. Popular urban medical myths often preach that all gluten is evil. I very much disagree.
Historically, grains were an important part of our diet — especially less refined grains. Our microbiome tend to do better with grains, especially oats and barley.
Fundamentals
Different cereal crops have different gluten. This may be very important with ancestry from the United Kingdom, Scandinavia, Poland, Russia, Baltic states. Before the genetic manipulation of wheat, there was a “wheat line” across Europe. North of it, wheat did not grow/was not cultivated. Wheat’s gluten was foreign to the microbiomes and DNA of people living there. Wheat has had a massive DNA history with historic Chinese wheat being very different than Spanish where (see this article). Wheat has been massively manipulated over the decades.
Gliadins found in wheat, which have three main types: three main types of gliadin (α, γ, and ω). Each has different amino acid sequences.
Hordeins found in barley, which have with major grouping B, C, D and γ [2009]
Secalins found in rye, which has γ and ω groups [1983]
Several later studies (Srinivasan et al., 1996; Janatuinen et al., 2002; Kemppainen et al., 2007; Guttormsen et al., 2008) indicate that oats are not unsafe for those with Coeliac disease (CD), and thus oats are now often included in the CD diet (Butt et al., 2008; Guttormsen et al., 2008).
If you “react to gluten” or “feel better without gluten”(which may be an induced placebo effect), there are dozens of different chemicals falling under the gluten label. You should attempt to isolate which ones are problems. Wheat gluten is something that I personally minimize, because all of my ancestors were above the wheat line — dark solid rye bread, rye crispbread were what they had. Wheat flour was an imported luxury. Oat and Barley porridge for breakfast was also traditional.
Cutting all gluten from your diet is likely very unhealthy to your microbiome. Even if you have Coeliac Disease, you should try barley and oats porridge (beware of buying from “bulk” – cross contamination is very common using bulk bins).
With the announcement that uBiome is asking to change from a Chapter 11 (Reorganization) to Chapter 7 (Shut the doors!) – the question is what comes next?
During the company’s Chapter 11 filing, the company had indicated that it would be looking into a sale. However, according to the motion it filed in court today, the company wasn’t able to secure lending that would enable it to continue operations. As a consequence, it has requested the court allow it to cease operations and liquidate its assets in order to pay off its creditors. The bankruptcy court still needs to approve the motion. If it is accepted and the company moves to Chapter 7, the liquidation of uBiome’s assets will happen under the supervision of a court-appointed trustee.
At this point it becomes interesting — superior technology than what ubiome (also thryve, and American/British Gut) is available. There are two on interest because they are using superior technology
XenoGene – they do have viable downloads available (just uploaded some tonight by data scraping their PDF files) and my contact with them indicates they are going to be making an upload friendly version available soon
What is the difference between technologies…. well with the older technologies we are talking 400-600 taxonomies. The last XenoGene that I uploaded had over 6000 taxonomies – a factor of 10 more! This was 182 pages of data with one taxonomy per line. This does come at a cost 10x more — but I expect the price to come down rapidly. There is a market out there… the fact that it appears that 1.4+ million samples have been processed by uBiome means that opportunity is there, a $140 million dollars of potential sales!
To me, Xenogene has set a new gold standards for retail microbiome reports.
The company that grabs this opportunity, the vacuum left by uBiome may be in China, Russia, Israel, India, Denmark, Australia or Spain. Setting the right price point, picking the right equipment and designing a good friendly user site is the key.