A reader wrote today: “One thing that maybe you can comment on. Xifaxan did not show up and is the new standard for SIBO treatment. Any insight? “
I am going to do a walk through of how those of you without brain fog could do it. [Hint: I do not want to have hundreds of request to do it for other things – this reader got lucky with asking the right new question!]
First we need to decipher the trade name Xifaxan
XIFAXAN tablets contain rifaximin, a non-aminoglycoside semi-synthetic, nonsystemic antibiotic derived from rifamycin SV. Rifaximin is a structural analog of rifampin. The chemical name for rifaximin is (2 S,16 Z,18 E,20 S,21 S,22 R,23 R,24 R,25 S,26 S,27 S,28 E)-5,6,21,23,25-pentahydroxy-27- methoxy-2,4,11,16,20,22,24,26-octamethyl-2,7-(epoxypentadeca-[1,11,13]trienimino)benzofuro[4,5- e]pyrido[1,2-á]-benzimidazole-1,15(2 H)-dione,25-acetate. The empirical formula is C43H51N3O11 and its molecular weight is 785.9.
rxlist.com
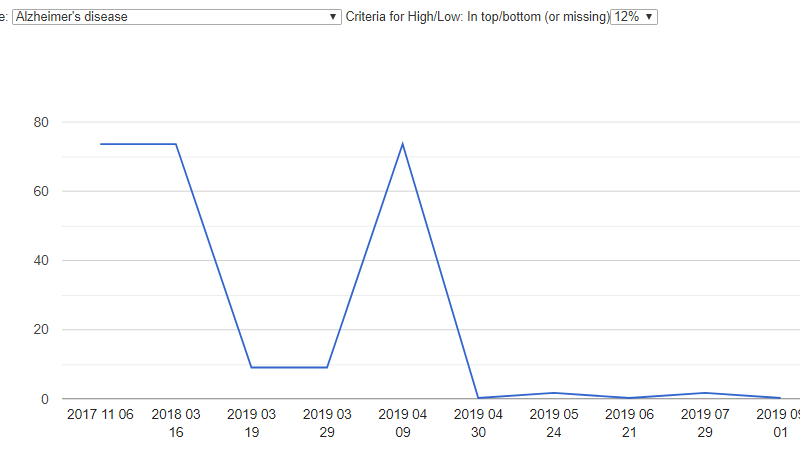
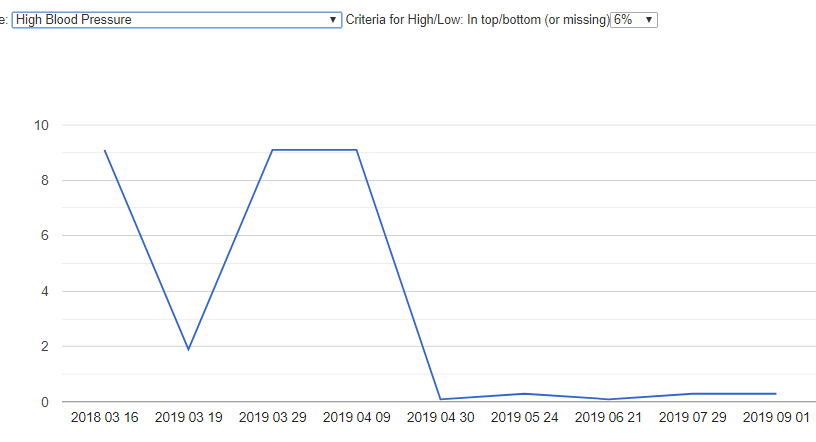
The next thing is to see if we have any information on these two – for xifaxan we have none, for rifaximin, we find it on our full list of gut modifiers that we have some information on. It’s link is here.
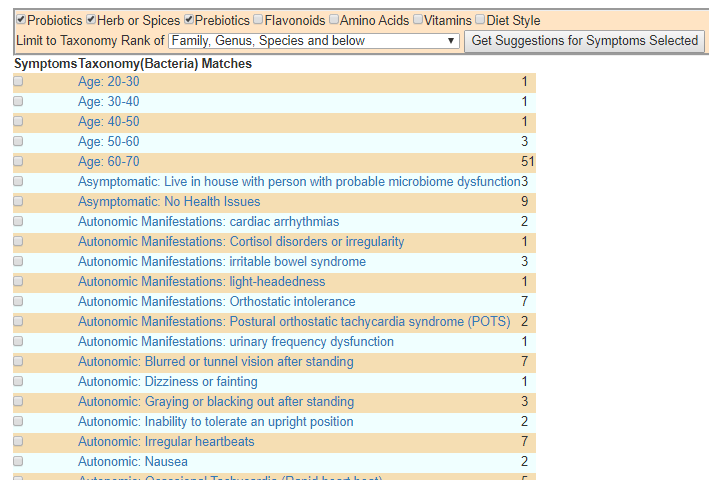
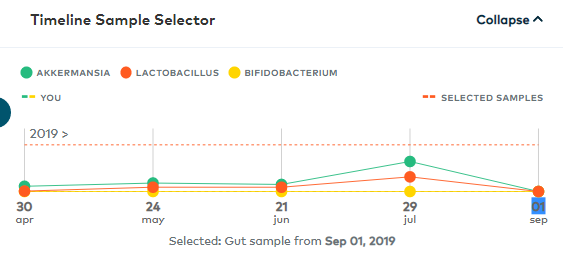
The second side of the question is microbiome shift for SIBO. We have two extremely high associations (in yellow) and a ton of associations < 0.05 (5% chance of happening at random — almost all at the high end!). I am extremely conservative in declaring significance.
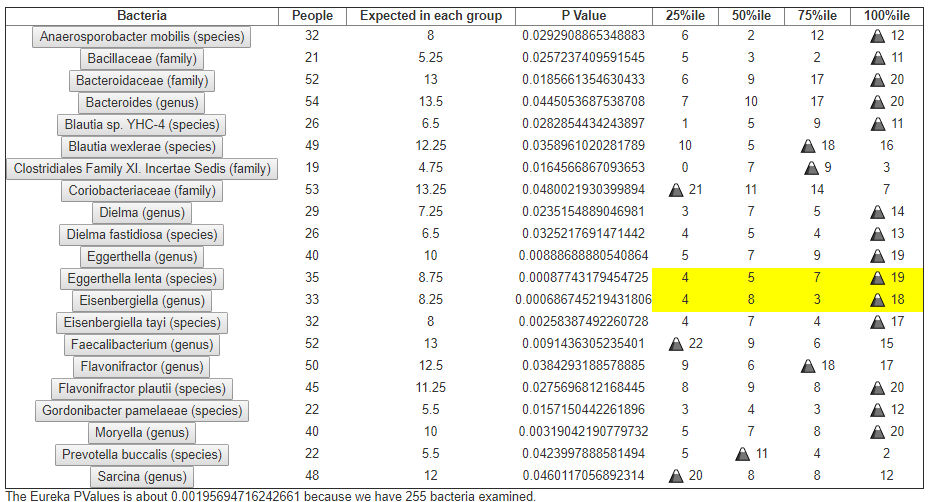
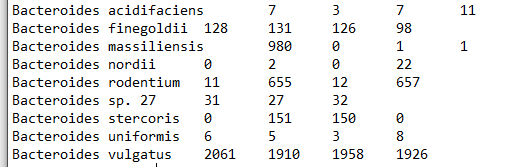
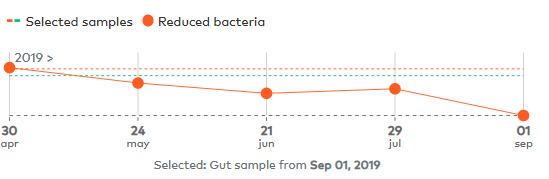
The next step is easy: comparing the two lists and seeing where there “is apparent agreement”, that is, xifaxan reduces a high bacteria (or encourage a low one).
- For the Eggerthella and Eisenbergia genus — there appears to be no impact.
- Similarly no impact for Moryella, Flavonifractor, Dielma, , Sarcina
- In terms of parents of species: Nothing on Gordonibacter,Prevotella, Anaerosporobacter
- It does decrease Bacteroides
- It does decrease the parent of: Blautia
Where do we get this information?
The key information is summarized on the above page (with links to the source — definitely open medicine!), but to illustrate for the casual reader:
- Review article: the antimicrobial effects of rifaximin on the gut microbiota. Alimentary pharmacology & therapeutics (Aliment Pharmacol Ther ) Vol: 43 Suppl 1 Issue Pages: 3-10 PubDuPont HL : 2016 Jan Epub
- Modulation of the gut microbiota composition by rifaximin in non-constipated irritable bowel syndrome patients: a molecular approach Clinical and Experimental Gastroenterology (Clin Exp Gastroenterol ) Vol: 8 Issue Pages: 309-325 Pub: 2015 Dec 4 Epub: 2015 Dec 4
Inference from above
It does not move anything is the wrong direction :-). However, it only impact 18% of the bacteria shifts at the genus level. I would expect that it would result in statistically significant improvement of a study group with enough data massaging. No remissions should be expected.
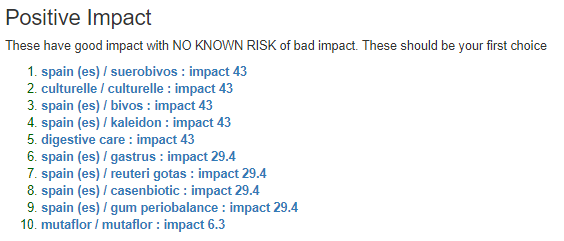
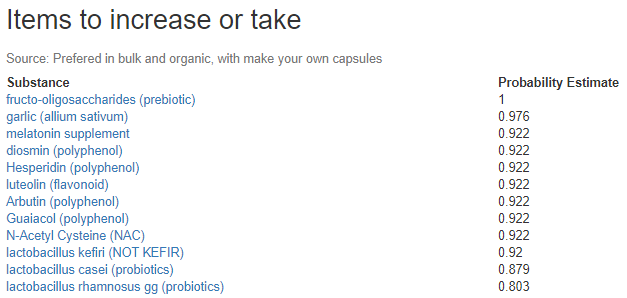
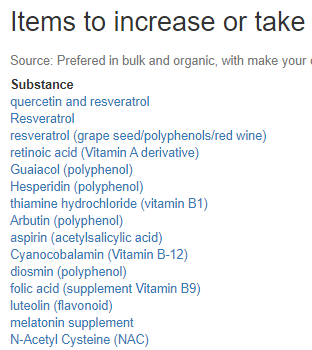
Would I take it? No, I would first try the following:
In fact, doing a little behind the scene magic (by adding modifier=P,A,D to the url), the following may be more effective (and definitely off label)
- Emtricitabine
- Naproxen – Pain
- Atenolol – High Blood Pressure
This latter approach is hunting for drugs based on reported microbiome changes; then evaluating safety and side-effect risks.If you have a condition that could warrant being prescribed them, you may wish to negotiate with your physician on a change of prescription.
Actual Studies?
- ” Response rates to rifaximin (550 mg three times daily for 14 days) were 47.4% for hydrogen positivity alone and 80% for both hydrogen and methane positivity. ” [2019]
- ” Rifaximin was not effective in improving IBS symptoms and QOL in GW Veterans with non-constipated IBS. ” [2019]
- ” Rifaximin therapy is well tolerated and the results are promising in terms of efficacy in eradicating small intestinal bacterial overgrowth in CF. ” [2019] “promising” is double talk for no statistically significant results but we are not willing to give future grant money to do more studies.
- ” Combination of amoxicillin and rifaximin may be effective in the treatment of patients with small intestinal bacterial overgrowth syndrome and concomitant H. pylori infection. ” [2018] again “may be” means that they did not get statistically significant results.
So, studies appear to support my logical conclusion using the model and our citizen science data.