“Two papers published earlier this year showed that people with chronic fatigue syndrome – also known as myalgic encephalomyelitis, or ME/CFS – have less of a gut bacterium called Faecalibacterium prausnitzii “
The following are permissible extracts (200 words per article). Click [more] to read more…
How the microbiome changes our idea of what it means to be human
YOU may, quite reasonably, think you are an individual of the species Homo sapiens. Once you have finished reading what follows, you will hopefully have been convinced that there is far more to us than that. Trillions of other organisms live on (and, more notably, in) your body. As you will see in the reports that follow, their impact on you is such that you will probably never think about yourself in the same way again. Your microbes change who you are and what it means to be you. With knowledge of this facet of ourselves growing rapidly, exploring it has never been more relevant.
Until recently, scientists believed that there were three discrete parts of our nature that reflected solid aspects of an individual self: the immune system, the genome and the brain. “None of these pillars of the traditional definitions of the self – immunity, genome integrity, the central nervous system – are free of microbial impact,” says Thomas Bosch at Kiel University in Germany.
The microbes that colonise us, collectively known as the microbiome, challenge the concept of a discrete self. These include bacteria, viruses and fungi, although the bacteria are the best-studied. [more]
The best way to care for your microbiome to keep it healthy as you age
Your gut microbiome is a vital support system for mental and physical health, supplying the body with all-important nutrients and helping tune the immune system.
As we get older, the balance of microbes in our gut changes. There are declines in beneficial types, such as the anti-inflammatory Faecalibacterium, and an increase in species that lead to more inflammation, which is implicated in multiple age-related conditions, including heart disease, cancer and cognitive decline. Many studies, with participants ranging from an isolated rural population in India to a wealthy semi-urban community in Italy, show striking similarities in the microbiome signatures of old age. One key finding is that people who have no significant health concerns in older age have an abundance of distinct beneficial microbes that are lost when there is a shift to physiological decline.
It isn’t clear whether the microbiomes of healthy older people are driving their vitality or are a result of the way they live, but an astonishing study in mice by John Cryan at University College Cork, Ireland, and his colleagues found that transplanting gut microbiota from young animals to elderly ones reversed age-associated impairments in brain function. [more]
Can probiotics and supplements really improve your gut microbiome?
If you have a condition like irritable bowel syndrome (IBS), a finnicky gut or just want to keep your microbiome in top condition, you might be tempted by products and treatments that offer a microbial tune-up. But what really works? Here are the main tools to engineer a better gut.
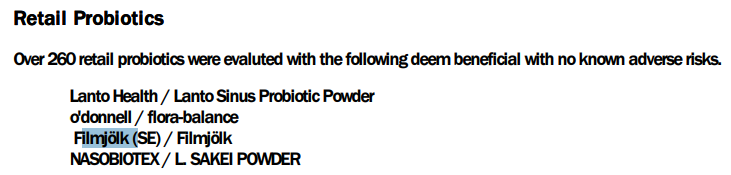
Probiotics
Probiotics are microbes that may help to restore healthy gut microbiota. If they also improve your mood, they are called psychobiotics. You can typically get them from eating naturally fermented foods like yogurt that contain beneficial bacteria, such as Lactobacillus or Bifidobacterium.
But as an adult, these microbes are unlikely to colonise your intestines. To the extent that they are helpful, their benefit comes while they are passing through. Such probiotics stimulate immune cells in the gut to reduce inflammation, increase mucus production and deter pathogens by producing lactic acid. But as mere visitors, they need daily top-ups.
Probiotic supplements have been used (with mixed success) for more than a century to help with the gut conditions of Crohn’s disease, colitis and IBS. They have also been shown to help with weight loss in people who are overweight and are increasingly being used for other conditions… [more]
Secrets of a long and healthy life reside in your gut microbiome
WHY do we age? As youngsters, we seem invincible. We climb trees, frolic in the dirt and blithely share alarming quantities of mucus. At college, we can thrive on a diet of ramen and beer, party all night and still sit an exam the next day. But in our 30s, we start to wind down. It becomes harder to maintain muscle tone and avoid illness. Our joints start to ache and our memory begins to dim. And it is mostly downhill from there.
People have long attempted to stop or reverse this process. But fountains of youth and secrets of immortality remain firmly in the realms of fiction. Our bodies wear out, even if we no longer do the back-breaking physical labour our ancestors did. And the world seems determined to grind us down with a plethora of disease-causing microbes. To help fend off these pathogens, our bodies recruit other microbes, vast numbers of which reside in our intestines, where we feed them in exchange for their services. But, as we age, this gut microbiota becomes less effective at fighting diseases too. [more]
Where does your gut microbiome really come from – and does it matter?
Imagine a remote island, recently formed by volcanic activity, in the middle of the ocean. At first, it is lifeless, but a growing variety of plants take hold, providing food for pioneering animal species, until eventually there is a diverse and flourishing ecosystem.
This is a useful way to think about how our gut ecosystems develop. “Your microbiome goes on a journey,” says Alan Walker at the University of Aberdeen, UK. “When you’re born, some bugs get in and then, when you start eating solid foods, other bugs replace them. There’s a dynamic process where your microbiome changes until you get to mid-to-late childhood. Then, through adult life, you’ve got a reasonably stable microbial community.”
Does a C-section affect a baby’s microbiome?
The first individuals that colonise an island can have long-lasting influences on its ecosystem, an idea known as the founder effect. Until recently, the thinking went that if the founder bacteria in a baby’s gut were unusual – because the baby was born by Caesarean section, for instance – this might disrupt their bacterial ecosystems. This idea has led some parents to take radical steps to get their children’s microbiomes back on the right track. [more]
What is the role of the microbiome in diseases like chronic fatigue
ONE of the most compelling discoveries about the gut microbiome is its influence on the immune system. Between 70 and 80 per cent of immune cells are in the gut, where they are constantly communicating with microbes. This crosstalk helps fight disease, strengthen immune responses and regulate inflammation, our body’s first line of defence against infection. Controlling inflammation is critical, as too much damages cells and helps drive chronic illness.
It is no surprise, then, that a growing body of evidence implicates the gut microbiome in various chronic diseases, from arthritis to Alzheimer’s. It is still early days, and most of these findings only point to associations. But they raise the possibility that gut microbes may contribute to, or even cause, some of our most intractable conditions, an idea that has already inspired new treatments.
It is now well established that gut microbiomes in people with conditions like multiple sclerosis, type 1 and type 2 diabetes, Parkinson’s disease and even asthma differ significantly from those of people without an underlying illness. Two papers published earlier this year showed that people with chronic fatigue syndrome – also known as myalgic encephalomyelitis, or ME/CFS – have less of a gut bacterium called Faecalibacterium prausnitzii [more]
How your microbiome is shaped by your friends, family, lovers and pets
When we are born, we get most of our gut microbes from our mothers (see “Where does your gut microbiome really come from – and does it matter?”). But as we get older and form other close relationships, including with intimate partners, friends and pets, we start to pick up their microbes too. This could potentially affect our risk of developing conditions like obesity, inflammatory bowel disease, asthma and allergies (see “What is the role of the microbiome in diseases like chronic fatigue?”).
“I jokingly say that your dating app profile should include your microbiome profile,” says Brett Finlay at the University of British Columbia in Canada.
The strongest evidence comes from work published in January by Mireia Valles-Colomer at the University of Trento, Italy, and her colleagues, who conducted the largest study to date of how our gut microbiomes are shaped by the people around us. They analysed DNA in the faeces of more than 7000 people from households around the world, including rural parts of Africa and South America and cities in the US, Europe and China, to find out which bacterial strains were in their guts and what proportion they shared with others. [more]
—————– from older issues ———————-
Your gut microbiome is linked to your fitness and biological age
The diversity of microbes in the gut could affect a person’s fitness and their biological age. Better understanding this may one day lead to probiotics that alter the gut’s microbial make-up to promote health.
Zsolt Radak at the Hungarian University of Sports Science and his colleagues studied 80 amateur rowers, aged 38 to 84, who participated in the 2019 World Rowing Masters Regatta in Velence, Hungary.
The rowers, whose training regimens ranged from practising every day to once a week, each provided a stool sample to identify the bacteria in their guts. The researchers also took blood samples to gauge the participants’ biological ages – a measure based on DNA markers, rather than the number of years someone has been alive.
The researchers found that having higher levels of gut microbiome diversity was linked to lower levels of fitness and an accelerated rate of biological ageing. This somewhat goes against previous research that linked lower gut microbial diversity to conditions such as obesity and type 2 diabetes. [more]