A reader message me with a drug that I was not familar with
Hello, my brother has CFS and I would like to ask you a question. We talked to a doctor at the ‘…..’ hospital in Germany who specializes on CFS. The doctor suggested taking Pyridostigmine bromide. What are your thoughts on that?
This is a drug that I am not familiar with and thus interested in finding out more.
First, what is it’s typical use:
Pyridostigmine bromide (PB) is a drug used during the Gulf War as a pretreatment to protect troops from the harmful effects of nerve agents. It has been used for more than 40 years in the routine treatment of myasthenia gravis and may be used following surgery in the reversal of neuromuscular blockade (Williams, 1984).
So, if the brother had been involved in the Gulf War, there seem to be some logic to this suggestion. However, constructive logic usually have risk and is inferior to doing research. What I found sent my air-raid alarms sounding.
Results indicate that more than 21 PyridostigmineBromide (PB) pill exposure was associated with consistent reporting of fatigue, pain, and cognitive/mood symptoms as well as the development of six additional symptoms over time. Veterans reporting exposure to more than 21 PB pills were more than 8 times as likely to consistently meet the criteria for Chronic Multisymptom Illness over time.
A reader pointed me to Mestinon on ME-Pedia.org which presents some interesting reads. My ground rules have always been to rely on gold standard sources, that is, peer-reviewed PUBMED articles.
My typical reading of OLD thin results is that there were follow up studies that showed no effect or negative effects, hence never submitted for publication (or not accepted by publishers).
Revisited PubMed
PubMed failed me because it did not find this drug by alternative names…
This was a single dose test. “Pyridostigmine improves peak Vo2 in ME/CFS by increasing cardiac output and right ventricular filling pressures. Worsening peak exercise Vo2, cardiac output, and right atrial pressure following placebo may signal the onset of postexertional malaise. “
Bottom Line
I would declined, and actually ask the doctor for published studies that shows it would help. The evidence is that it would make the symptoms worst. A single dose appears to help, the evidence of the cumulative effect of multiple doses are a worsening of the symptoms.
This is one of the few cases that I would consider writing to the licensing authorities if the doctor response to being presented with the above information is arrogance.
For your brother, I would suggest getting an appropriate microbiome test (being in Germany, my choice would be BiomeSight.com from the UK), and using “Dr. Artificial Intelligence” at https://microbiomeprescription.com/ . Dr.A.I. fees are reasonable (free), with immediate availability once you get the test results. So far the feedback from people using him has been very positive.
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
Dr. A.I. is not a person ,it stands for Artificial Intelligence – a compute program that takes facts (in this case, well over 10 millions) and use logic to come up with suggestions based on probability.
Back Story
34 years, male with ME for around 4 years.
My lab tests are usually normal, with the exception of :
elevated calprotectine (130mg) tested in 2020
cholesterol has always been very low, and I’ve been VERY skinny since I was a kid (I’m now 59kg for 183cm, no matter how much I eat)
Vitamin D used to be very low but now in normal/upper range
Gamma-globulins always come back slightly elevated (around 14 g/L)
Bilirubin always a bit high
Sugar in blood always a bit too much high, even when I don’t eat sugar for extended periods
I’ve had a PET/IRM scan 6 months ago which showed “moderate hypoperfusion” in some parts of my brain.
Back story :
I’ve always needed more rest than other people even when I was a kid/teenager but I could live a somewhat normal life until 4 years ago. I had chronic sinusitis as a kid which got better after I had sinus surgery when I was 16 years old, and I had to take antibiotics all the time when I was a kid. I’ve caught a staphylococcus aureus at that time and I was tired but I got better. As an adult, I used to work full time as a jazz musician and music teacher. I started getting more and more tired and couldn’t keep up with the concerts anymore and thought it was because of the unusual schedule, so I’ve decided to switch to web development. At this time, the following symptoms appeared gradually :
brain fog
glassy eyes and eye discharge in the corner of my eyes that I have to wipe off several times a day
face red and swollen around the nose (I’ve thought of lupus but my auto-immune markers are just a bit too high, which didn’t worry doctors)
headache in the back of the head and around the neck (probably because of hypoperfusion or thick blood)
diarrhea or greasy stools almost every day. I’ve had that one for many years prior to my CFS though.
I didn’t understand why I was so tired and thought that I just had to keep going, and started to exercise more. I remember going to the pool or doing kendo and I was coming back extremely exhausted and brain fogged, thinking that I would eventually get better. I’ve started to see many doctors and thought that my problems came from my gut, because there were so many foods that I couldn’t digest, and my body seems to be unable to process fat. I’ve discovered that I had the parasite giarda intestinalis. I don’t know when I’ve caught this, but it went away with antibiotics (I can’t remember the name). I also had my wisdom teeth removed prior to the beginning of my ME/CFS and the doctor said that my teeth were very difficult to extract. I’ve had an infection in one of the cavities 2 or 3 days after the surgery, that went away with another round of antibiotics. I also had a violent car accident at that time and was very lucky to come out of it with no injury, but my body was very tense for a long time. All of these things happened around 4-5 years ago. Since my gut issues didn’t get better, I’ve finally had a colonoscopy which showed nothing special. My ME/CFS gradually worsened over time and I’ve only been able to work 8 months as a web developer. I grew more and more tired everyday and I had to take quick naps in the toilets whenever I could. I finally couldn’t keep up and had to stop. It’s hard to stay where I stand on the fatigue scales because I’m able to exercise (I could run 30 minutes now) and I don’t feel pain in my body, but the brain fog is very heavy. My ME/CFS was at the worse point around 1 year/6 months ago. I felt extremely tired, and I could crash from just talking to someone over the phone for 10 minutes and couldn’t play a video game, but I was still able to go for long walks. I had troubles breathing though. So my symptoms are mostly what I call my “brain inflammation”, the diarrhea, the eye discharge and of course the crushing fatigue. I’ve recently been diagnosed with ADD, which I guess I always had, but the “ADD symptoms” are much worse since I had CFS. I’ve started taking Ritalin in small doses very recently, which helps me focus a lot, and feel almost normal for a couple of hours.
I’ve started taking tons of supplements around 6 months ago and I’m in a better place now. Here are all the things I’m taking :
Paroxetine 10mg
Acetyl L-Carnitine
NADH
Ubiquinole
R Lipoic Acid
B12
A B-Vitamin complex
Vitamin D
I’ve tried low dose Naltrexone but it made me much worse.
I’ve also discovered your website and your work at that time, and did my first microbiome analysis in february. I was very heavily brain fogged so I think I didn’t use the prescription website properly, but I started taking these :
Licorice (Spezzata)
Slippery Elm
Triphala
Dark chocolate
Turmeric
Nattokinase
Grape Seed Extract
Lots of garlic in my food
I’ve also added Rhodiola Rosea, which gives me motivation and energy to do things, but its effect is much more subtle now.
I’ve started to get slowly (not so slowly actually) better since then. 6 months ago, people had to help me clean my house or do the groceries for me. Now I’m able to study coding a little bit, go out with my friends, do short trips, etc. I’m thinking about going back to work, but since brain fog is still my very worst symptom and since mental exertion can really make me crash, I’m not sure about this.
I’ve started taking Selenium (400mcg) very recently, which seems to help. I’ve also been experimenting with nicotine gums.
Regarding sleep, I can sleep like a baby around 9 hours per night but I don’t feel rested when waking up. I grind my teeth very hard at night, but it’s better since I have a mouthpiece.
I’ve had a second microbiome analysis done in May and would love to have your input on this. I’m surprised that my microbiome has changed so much and I even wonder if there isn’t some kind of error ! That would be great if you could help me target which bacterias I should focus on for the next few weeks. Anyway, thanks a lot for your work, I’m in a better place now and it’s mostly thanks to you. I just hope I can get the last 20-30% of energy back so I could go back to work and live a somewhat normal life.
Analysis
This person has two samples, so we will look at what changed between samples.
The earlier sample had a strong over representation of rare bacteria which had improved greatly by the second sample.
Feb 10, 2022 (upload date)June 20,2022 (upload Date)
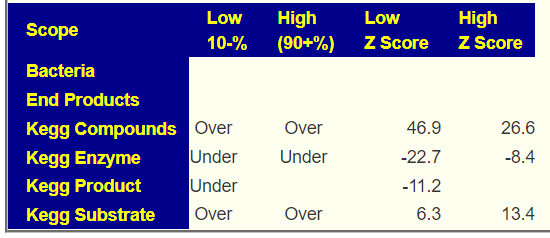
Looking at the new [Research Features]/Over and Under Population, we see KEGG compounds flip from over representation to under representation — this means that compounds are shifting to the middle/normal between. Under representation should be viewed as good because it means that we have less over production or under production occurring. Kegg Substrate is a measure of bacteria consumption, being over implies an imbalance.
Feb 10,2022June 20,2022
Looking at Health Indicators, we seen an increase of bacteria deem unhealthy between the samples, but the only ones that stands out is Corynebacterium and several streptococcus( Streptococcus anginosus, Streptococcus vestibularis). Dr. Jason Hawrelak Criteria stayed at 89%ile for both samples.
Top Probiotic suggest enviromedica terraflora sbo probiotic (was #3 on earlier sample) with the Weight dropping from 4226 to 2.5. A drop in weight indicates less shortage of what the probiotic provides.
Dr. Artificial Intelligence Suggestions appears to have worked
Remember, the suggests are items computed to reduce the severity of symptoms by adjusting the microbiome. This story (and several other emails/comments that I got this week) seems to validate the hypothesis that manipulating the microbiome based on retail microbiome tests (with the right AI) works. It may not be overnight, it is a slow progression. It is a progression.
The Road Forward
Manually inspecting [My Profile]/Visualizations/Microbiome Tree, I checked items with a count over 2000 and flag as too high for a hand picked selection, he had multiple types of bifidobacterium (good, but one was possible concern, Bifidobacterium gallicum, there is little literature on it). I noticed that almost all of the items flagged were blue (too many). A total of 39 bacteria was selected!!! Another one that stood out was Lachnospira (which went from 10% to 4.3%).
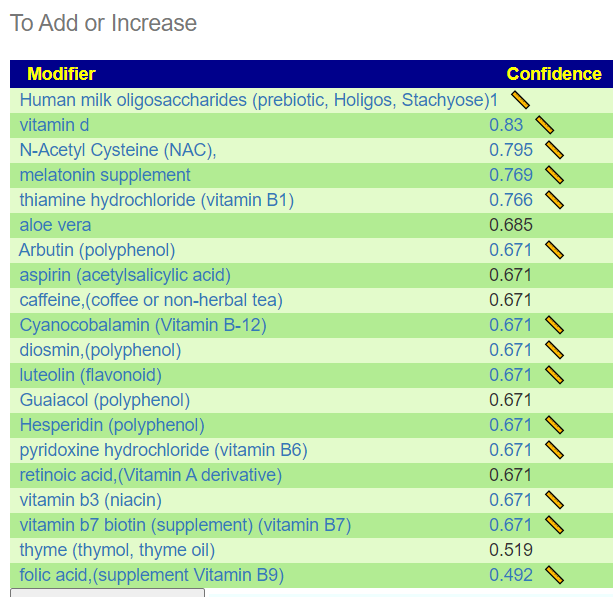
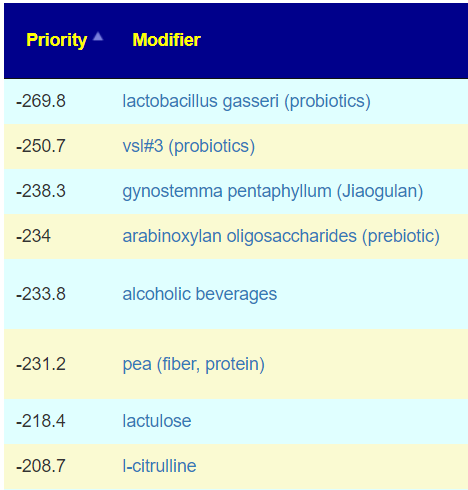
The results of this first run is below. Most of the items listed are items that have been shown to help many ME/CFS people in studies. Diosmin with hesperidin is available as a supplement (from citrus fruits) and there are no studies on PubMed for either with ME/CFS, thus a potential novel supplement for ME/CFS.
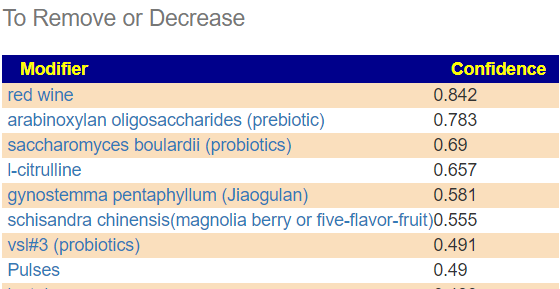
The avoid list is also interesting… avoid red wine — very much standard advice for ME/CFS. Several probiotics are also listed. Note that there was no probiotics on the above list. This is not unusual for microbiome suggestions for ME/CFS (and some ME/CFS conference notes suggests that some MDs found probiotics are not helpful)
Next we do the usual building of consensus suggestions.
Percentile in top or bottom 10 % – 204 bacteria picked!!
The results were very similar to that of hand picked bacteria:
Take Items
And the avoid list was also similar
I attach the download below
Probiotics
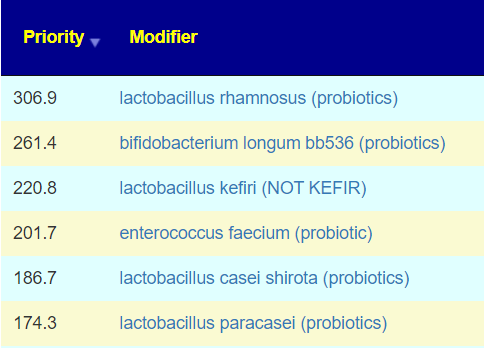
The top probiotics are shown below (remember those above were based on bacteria genes, those below on clinical studies, they would compliment each other).
Remember to rotate probiotics (after one bottle, or a month – which ever comes first). One of their key features are the “natural antibiotics” they produce. They effectiveness will drop off over time, by changing you will inhibit those bacteria that are resistant to the first probiotic.
Pick probiotics based on availability and cost (buy cheapest first!). For example, very few countries sell lactobacillus Kefiri. Lactobacillus casei shirota is sold as Yakult probiotic drink in many countries. See this page for appropriate dosages (often dosages on the bottle are too low to make effective change).
Personal Note
This person wrote “I just hope I can get the last 20-30% of energy back so I could go back to work and live a somewhat normal life.” Rushing back to work too soon is setting yourself up for relapse. Both times that returned to work after being disabled with ME/CFS I went slow. In fact, I spent 4 months as a volunteer developer for an organization — at first just 2 hours a day and slowly working up. Once I could handle a 40 hr work week fine, then it was very very careful job hunting…. you want a place with laid-back tolerate management that do not have venture capital overlords! The line that I used was this “I am recovering from a complex illness and expect full recovery, but for the next few months I may not be able to work every week full time, most weeks — YES. My MD wants to keep stress low on me during recovery.”
What about my frequent suggestion for ME/CFS?
This is seen in many analysis (including my own) — but every microbiome is unique. Never assumes what help Peter and Paul will help Mary.
In this case, “daily barley porridge with walnuts” is a definite no-no.ME/CFS is a dysfunctional microbiome — with each patient microbiome being different. I avoid making any suggestions for ME/CFS independent of an individual microbiome — this is likely why it is so hard to treat using cookbook recipes.
Barley is negative
Oats is negative
Walnuts is negative
Foods that are high priority are: soy, whey, eggs, banana, Konjaku flour (Konjaku noodles are available on Amazon).
Brain Fog
My working model is that the root cause is hypo perfusion, i.e. low oxygen delivery to the brain. There are several possible causes, the most likely are inflammation and hypercoagulation. With ME/CFS sibling, Long COVID, there is a lot of recent studies citing “micro clots” — an alternative term for hypercoagulation.
I did a summary of if back in 2016, Hypercoagulation and the Microbiome. My hypothesis is that the triggering of inflammation or hypercoagulation is due to a mismatch of compounds produced by the microbiome. I just realized that from the uploaded samples, I may have sufficient data to identify some suspects — but that is for another post.
At the moment, my experience has been that the following non-prescription items help
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
Back Story
Typical for ME/CFS, fatigue and brain fog prevented much of a backstory. Fortunately, she was able to complete symptoms — which gives a good back story and also shows overlaps with many others:
Neurocognitive: Brain Fog [482 samples]
General: Fatigue [442 samples]
Sleep: Unrefreshed sleep [388 samples]
Neuroendocrine Manifestations: worsening of symptoms with stress. [367 samples]
Neurocognitive: Difficulty paying attention for a long period of time [360 samples]
Neurocognitive: Can only focus on one thing at a time [341 samples]
Neurological-Audio: Tinnitus (ringing in ear) [331 samples]
Neurological-Audio: hypersensitivity to noise [309 samples]
Gender: Female [299 samples]
DePaul University Fatigue Questionnaire : Fatigue [297 samples]
Immune Manifestations: general malaise [295 samples]
Onset: 2010-2020 [285 samples]
DePaul University Fatigue Questionnaire : Unrefreshing Sleep, that is waking up feeling tired [268 samples]
Neurological: Difficulty reading [253 samples]
General: Depression [242 samples]
Post-exertional malaise: Worsening of symptoms after mild physical activity [230 samples]
Post-exertional malaise: Physically tired after minimum exercise [226 samples]
Official Diagnosis: Allergic Rhinitis (Hay Fever) [211 samples]
Neuroendocrine Manifestations: intolerance of extremes of heat and cold [208 samples]
Post-exertional malaise: Inappropriate loss of physical and mental stamina, [205 samples]
Official Diagnosis: Chronic Fatigue Syndrome (CFS/ME) [201 samples]
Analysis
Following my usual path My Profile/Overview found an over population of rare bacteria and under population of common bacteria. This is important to note because most clinical studies focused on shifts of common bacteria, and exclude rare bacteria (sample sizes and lack of sufficient statistical training are the typical cause).
Dr. Jason Hawrelak’s criteria came in at 56%ile, not any clear issues, with the following main items of note:
My first analysis in building a consensus report is hand picking the above and seeing the results.
The top items are similar to other ME/CFS suggestions and repeats my often refrain “Have barley porridge with walnuts” sweeten with sucralose for breakfast each day:
WARNING ABOUT GLUTEN-FREE MIS-INFORMATION
Research your science well:”Gluten is a complex mixture of hundreds of related but distinct proteins, mainly [in wheat] gliadin and glutenin. Similar storage proteins exist as secalin in rye, hordein in barley, and avenins in oats and are collectively referred to as “gluten.” ” What is gluten? (US National Library of Medicine) Barley is free of glutenins and gliadins, the troublesome glutens. You may be using “All black men are criminals” reasoning. You really need to be tested for which types of gluten proteins you reactive to and not go for internet-legend that all glutens are bad.
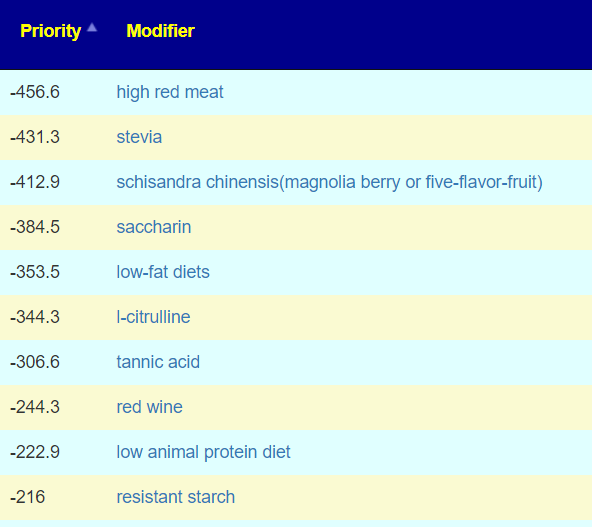
The avoid list suggests not to use soy milk with the porridge. Red wine for ME/CFS is a very typical avoid (most ME/CFS cannot tolerate wine… I wonder why 😉 ). Let us see how much consensus we get from doing the pro-forma consensus building
We go to Changing Microbiome/Consensus Suggestions
The person has entered their symptoms (see above). Unfortunately, there are many different paths that can be taken. The intent of picking bacteria by symptoms is to allow suggestions to be based on the most likely bacteria for the most troublesome symptoms for a person.
This is on Research Feature / Experimental /Build a Hand Picked collection using Symptoms. I went with the following for illustration purposes.
Picked Symptoms
Neurocognitive: Brain Fog
Onset: 2010-2020
Immune Manifestations: Hair loss
Neurological-Audio: Tinnitus (ringing in ear)
Neurological: Joint hypermobility
I used “Expected” settings and got the following list. All of these were items with low values,
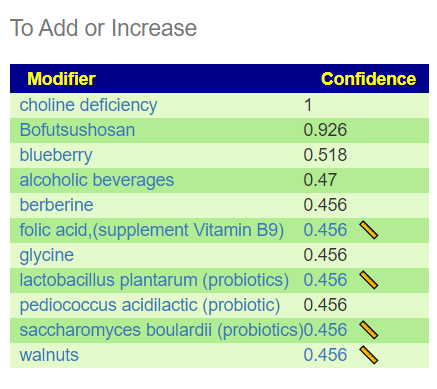
The suggestion list is very different than above:
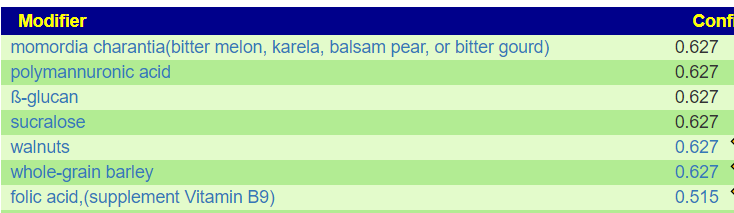
We see walnuts and for our morning porridge, add in blueberry. Bofutsushosan is very interesting because it increases AKKERMANSIA (mentioned above). I have done Bofutsushosan with Akkermansia probiotic and found a major increase in Akkermansia. Choline Deficiency means avoid foods that are HIGH in choline – see NIH List here.
The avoid list (items that will reduce the above bacteria) includes a number of probiotics:
Summing up probiotics
The following are my suggestions (2-3 weeks of doing one, then rotate to the next one)
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
I have done everything as planned since your first review
I maybe went up from 15% to 20%. I was able to reintroduce some new activities, but still am lying in bed most of the time. Also taking piracetam seems to help.
I still won’t be able to do the analysis myself.
COMMENT:ME/CFS patients are a priority for me because I personally understand their brain fog and cognitive impairments from past experiences.
I have had COVID in the meantime in case that matters for your analysis, but I did not notice any changes afterwards.
Analysis
Given the recent post for another ME/CFS person who had COVID too, with the result that their microbiome became a good match for long COVID and a poor match for ME/CFS, this was my first question. Fortunately, the sample was done via Biomesight, he did not needed with FASTQ files and transferring them. To keep the story short, I looked at his shifts compared to annotated sampled and compare to literature from the US National Library of Medicine nothing shifted between the samples. There is no shift towards Long COVID from ME/CFS in this case.
Comparing Samples
I do not know the answers. I have a model. Models often need adjustments so comparing samples (for better or worst) in a consistent manner is part of my learning process.
First thing we see a dramatic change with rare bacteria being seen much more often and common bacteria less often. There are more genus seen (184 vs 141) and more Species (230 vs 161) but this may be due the better sample reads in the latest sample (82,102 reads versus 55,117 reads).
Percentile
Latest Genus
Latest Species
Earlier Genus
Earlier Species
0 – 9
47
65
2
4
10 – 19
23
27
10
16
20 – 29
19
16
16
11
30 – 39
13
17
12
13
40 – 49
15
18
13
14
50 – 59
16
17
23
32
60 – 69
15
22
14
19
70 – 79
17
22
13
14
80 – 89
13
16
24
22
90 – 99
6
10
14
16
Average
18.4
23.0
14.1
16.1
Std Dev
11.0
15.4
6.2
7.4
Hawrelak’s criteria was 95.6%ile for both samples.
Potential Medical Condition dropped from 7 to 1. With Obesity being in common.
The person feeling subjectively better and doing more activities
Most of the other measures are the same or difficult to interpret. There is one possible concern, the high levels of Prevotella copri is an indicator of mycotoxin, typically from moulds and fungi. Considering that the time between the samples was winter with close windows and heating — there could be an environment issues here – so lots of fresh air may be good.
Over to Suggestions
There are various algorithms to suggesting probiotics, the strongest results are for:
I ran a few ways of picking bacteria based on Bacteria (and not genes) and lactobacillus casei kept was the top in the consensus report (overall and in terms of probiotics)
Unfortunately, some of the items have no studies. Given that the suggestions are based solely on bacteria with no knowledge of the diagnosis, the convergence with the literature suggests that the suggestions are very appropriate. Two different roads came to the same conclusion. In data science this is sometimes called “cross validation”. In Scotland, “O ye’ll tak’ the high road, and I’ll tak’ the low road, And I’ll be in Scotland a’fore ye,”
I looked at the antibiotic list for the latest sample and the top two are typically used for ME/CFS:
And interesting that several others often used are NOT recommended: azithromycin (which is a macrolide ?!?), minocycline [2021], fluoroquinolone, doxycycline.
ME/CFS is a heterogeneous condition with a wide variety of microbiome dysfunctions. I believe that using the microbiome to target the best candidate antibiotics is the rational way to proceed.
Question: Sadly I do not tolerate chocolate, but I will try it out again.
Answer: These are suggestions, do only what you are comfortable with. Nothing is required. The chocolate issue is interesting, my daughter does not tolerate most chocolates, she discovered that it was the type of sugar (i.e. made with liquid sugar / liquid glucose — adverse reaction) made with solid sugar — happiness. See Health effects of glucose syrup
If you try again, you may wish to determine the type of sugar actually being used first.
Question: Is there no avoid list?
Answer: Yes, in the download, any item with a NEGATIVE value in the priority is an avoid
Question: Is 1 capsule of Equilibrium per day really enough?
Answer: I honestly do not know. There is no literature to work from. If you take more, than separate them (i.e. 12 hrs apart)
Question: It seemed whenever I took turmeric that I was getting more nervous and anxious. Still take it now and then?
Answer: As above, do only what you are comfortable with — there are hundreds of items listed. Anxiety is contrary to the effects of turmeric / curcumin reported in the literature [2021] [2019] [2018] [2017]. If turmeric is causing die-off of bacteria that causes vascular constriction, that would result in anxiety. If you tolerate aspirin or niacin (flushing type), then try taking those with the turmeric.
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships.
Backstory of Latest Sample
In light of your recent few blog posts about uploads without many microbiome shifts to work with, I was thinking this could be a beneficial walkthrough video for what seems to be the opposite.
I was doing pretty well on my antibiotic rotations (mainly tetracycline two weeks on, two weeks off since Aug of 2021) until Feb or so when I had a major crash / flare that I’m still suffering from.
I did have a very mild case of Covid in mid January that felt no worse than a regular cold.
But from what little I can parse from this sample, it seems I may be struggling with long Covid. I say little, because my brain fog is extremely dense.
And all of the results I’m getting for this sample via your site seem so drastically different from what has been going on over the last 7 years (my oldest sample is from 2015).
Comparison of samples
This person has samples going back to 2015 using uBiome. Unfortunately for comparison we need to keep to the same lab (why? read The taxonomy nightmare before Christmas…).
Jason Hawrelak Criteria etc
We finally see an improvement with Jason’s criteria. We also may be seeing more diversity with the increase of Genus and Species found. I say may because this could be a side-effect of a low raw count in some samples.
Date
Percentile
Unhealthy Bacteria
Genus
Species
2022-04-11
98.8 %ile
8
220
303
2022-01-11
89 %ile
11
89
141
2021-03-09
89 %ile
8
108
153
2020-05-27
89% ile
7
153
223
Finally, we have a significant improvement
Expected values ar 10% for each line
I decided to look at the raw reads (which are captured from Thryve and Biomesights)
Sample Date
Raw Reads
5/27/2020
43311
3/9/2021
29247
1/11/2022
17630
4/11/2022
153194
The cause of the jumps above may be the number of reads from the sample
This lead me to look at what typical raw counts are from Ombre/Thryve
To find the raw counts for your sample, open the csv and look for this line
What is the consequences? It means that rarer bacteria may be ghost-like, appearing or disappearing from sample to sample. This adds let one more layer of fuzziness to doing analysis and generating suggestions.
First Question: ME/CFS or Long COVID microbiome or both?
This person uploaded the Ombre FASTQ files to BiomeSight so I may used data from the Long COVID study there. Both condition present similarly, I am curious to see if we have sufficient reference data to decide which condition is a better match.
Long Covid matches against Biomesight 154 SamplesME/CFS matches against Biomesight 62 Samples
We have concurrent matches for both both conditions
The table above hints that he is at present much closer to Long COVID than ME/CFS.
I am not sure about the political correctness of saying “Congrads! You no longer have ME/CFS, you have Long COVID!” is what the microbiome reads like.
What is interesting is that the microbiome constantly shifts/evolves, with Long COVID the infection is constant and the duration since the infection is short — hence less evolution of the microbiome over all patients. With ME/CFS the triggering infection possibilities are huge with 20, 30, 40 years of evolution of the microbiome — hence patterns are diffused by time and original infection.
Looking at deficiency of compounds produced, we see a dramatic drop from the previous sample suggesting that bacteria are getting the needed inputs for correct functioning.
Sample Date
1%ile
5%ile
10%ile
5/27/2020
4
14
60
3/9/2021
2
14
16
1/11/2022
197
233
244
4/11/2022
6
28
52
Kegg Compounds below %ile shown
Where do we go from here
I am going to do consensus, but do only 3 items:
Hand Picked Bacteria using the study in progress data using BiomeSight (16 bacteria)
Using US National Library of medicine filter to Long COVID using BiomeSight and Box-Whiskers (14 bacteria)
Using US National Library of medicine filter to Long COVID using Ombre and Box-Whiskers (14 bacteria)
The consensus is below as a download. Since antibiotics are being prescribed at present, I included that in the suggestions criteria.
Why did I focus on the ME/CFS ones? Path of least resistance for the prescribing MD – the MD accepts ME/CFS and thus will have low resistance to prescriptions often used for ME/CFS. Asking for them for Long COVID could get rolling of eyes…. As always, we are using these off-label for their computed microbiome effect. For the prescription items, I would suggest rotation (one item for 10 days, then a 0-10 day break, then another item (or repeat if limited to one item).