Why are the quick suggestions I get very opposite the ones from the advanced suggestions? soy is a top add in one and a top avoid in the other for instance. Many other similar situations.
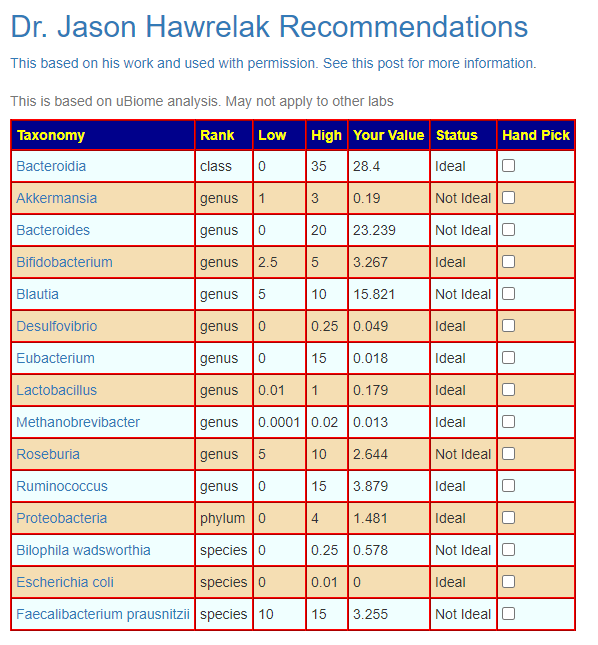
This is a good question. Quick Suggestions are based on the recommended ranges for a small group of bacteria from Dr. Jason Hawrelak, used with his permission. An example is below. This is not specific to any health issue.
For other suggestions, the bacteria picked determine the suggestions. Every bacteria has a different profile — so depending on which ones are selected, the suggestions will be different.
Some common ways of selecting the bactera:
Outliers – those too high or low compared to others. A crude method.
Bacteria which are high or low for a specific medical condition where your pattern matches
Bacteria which matches one or more symptoms where your pattern matches
Hand pick all of the bacteria using any criteria that you wish to apply.
We DO NOT KNOW what is the best way — it will likely be different for each person. We do not know which bacteria are “noise” and can be ignored in all cases.
If you look at the “Expert Consensus” page on your sample, you will see that there is disagreement. For some bacteria you will find some experts saying a specific level is too high and others for the same level saying it is too low.
I do not have a “safe suggestion” for anyone. I have built tools that allow various models of what is desired to be applied. I strongly recommend reading the following two posts to better understand the issues:
It means there are NO ABSOLUTE ANSWERS — they can never be…. it is like asking what is the height of a human (which varies by race and year of birth) and they asking what can I do to increase (or decrease) my height.
What you can get (especially if you are eating a ‘western diet’) is a feel of probable causes and things that will probably help. It has worked for me. It has worked for many readers who have tried it. Even in the face of “disagreement in technical details”, there can be strong patterns seen from the fuzzy data, see One Stool, Two Samples, One Lab — What the shit!.
You may wish to check my you-tube videos . I have plans to do a mini-course suite of them in the next few months.
A reader sent me the message below and gave permission to use his sample. I had, about a year ago, wrote The taxonomy nightmare before Christmas… that looks at the differences between lab results using the sample sample (as represented by a FASTQ digital file). We now try one more variation.
Last september I did (again) test my microbiome with Thryve. Because I had some general doubts about the validity of stool samples, I ordered two tests and took two different samples of the same stool and send them in under two different names. …the results confirmed my doubts as I got different bacteria levels of the ten strains Thryve shows in their overview.
STRAINS
% sample 1
% sample 2
akkermansia
0,2
0,4
alistipes
0,02
7,2
bacteroides
0,02
3,4
bifido
2,6
1
blautia
10,3
3,3
eubacterium
7,2
4,1
faecalibact.
1,7
11,6
lactobac.
1,1
2,2
roseburia
1,9
2
ruminococcus
26,6
13,8
So I do not doubt the reliability of each sample, but see that the validity of the sample is the problem. The results of a sample seem to be more or less random and not representative of the microbiome in general. …so I think that any advice given, based on the results of one sample is arbitrary. If we are to take the importance of the microbiome seriously, we will have to consider a new way of getting a representative sample to have a solid base for interventions concerning our health.
Sampling Statistics
The typical sample seems to contain a round a 100,000 bacteria and is usually reported out of a million (scaled up). “Bacteria in faeces have been extensively studied. It’s estimated there are nearly 100 billion bacteria per gram of wet stool. ” [src] The sample that you sent it was likely no more than one milligram.
To use the “if I was a Martian” model… It is like a spaceship abducting a boatload of people in the Mediterranean…. If the boat is a cruise ship full of fat diabetic elderly Americans you will get one result. If the boat are full of starving Nigerians children trying to become refugees in Europe, a very different result. That is a disturbing concept when you mind is fixed on a deterministic precise definitive result. It’s a sample folks! For most industrial processes, dozens (or hundreds) of samples are required to get quality assurance. For the nerds, some readings: [2015] [Wikipedia]
Example: Two employees working for the same company at the same job earning the same amount and living in the same community. You stop each of them and take a sample of how much money they have in their wallet. Would you expect them to have the same amount? Would they have the same number of pennies? dimes? quarters? Credit Cards?
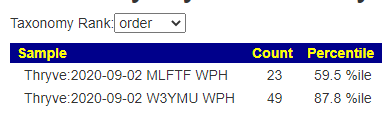
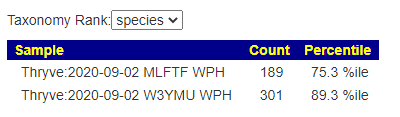
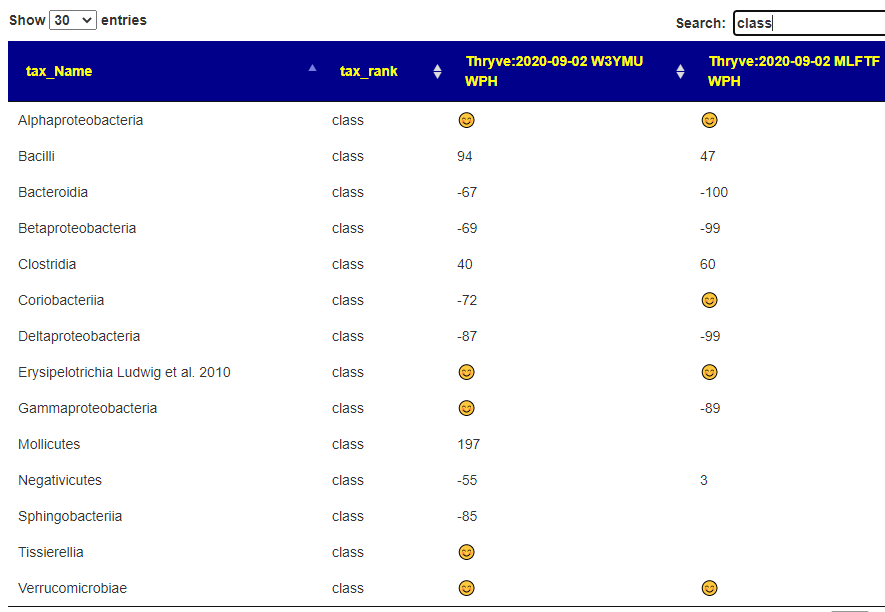
I would expect differences in samples to increase as you move down the rank. It is similar to asking at one level [European, African, Asian] on the abducted ship above. At the next level [Swede, Dane, Italian, etc] , the counts between sample will diverge as you do more detail classification.
This is an illustration on why I do fuzzy logic on predicting symptoms with good success according to readers. Using studies from PubMed have been reported to produce poor results according to readers.
When the two samples are used to predict symptoms, we have a strong convergence. While the actors may be different, their impact are similar.
Adjusting for Natural Variation
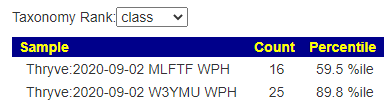
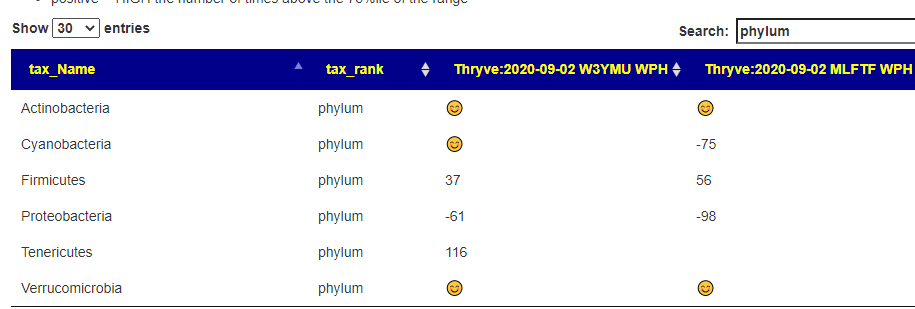
Using counts without context is a good way to get upset without justification. I use percentiles to provide context and have a comparison page (which I need to revise). At the phylum level we see general agreement between the samples. One rare phylum was lacking in one sample (not found in 30% of Thryve Samples but only 6% of BiomeSight – hint: download the FASTQ files and process them thru BiomeSight [for free!]).
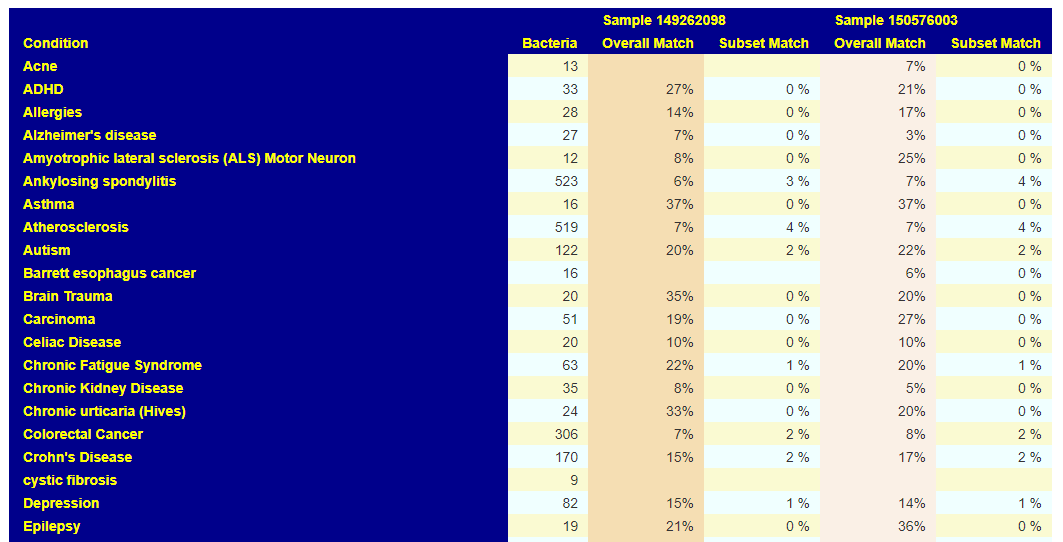
Medical Condition Matches
Going over to Pub Med Medical condition matches, we see a striking similarity between the samples as shown below. So for detecting medical conditions — they are almost identical to each other (despite the differences in bacteria)
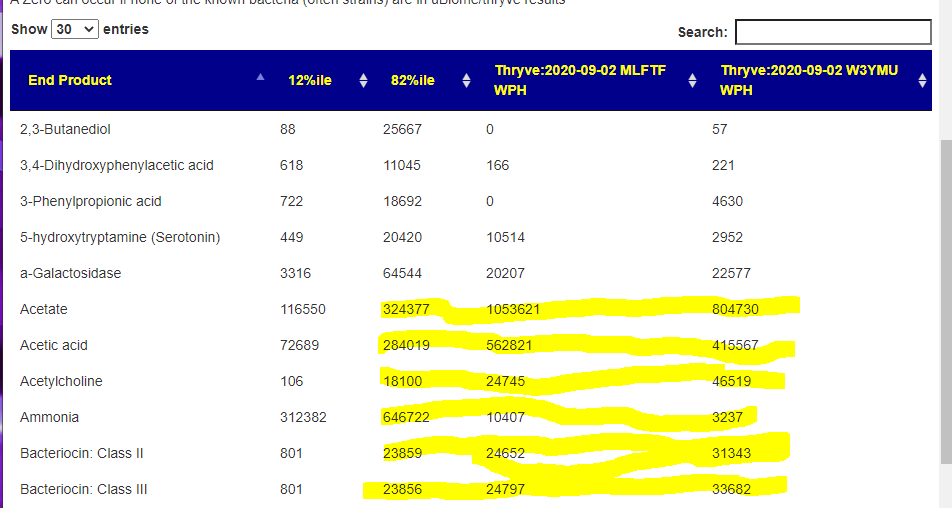
End Products Predictions
Again, we have strong agreement between the samples using 3 buckets.
Both below 12%ile (i.e. Low)
Both below 82%ile (i.e. High)
Both in normal range
This means for this type of diagnostic evaluation — they appear to be the same.
Bottom Line
There are several questions that need to be asked (and an answer to one):
To the folks at Thryve (and Biomesight.com), why are the numbers so different?
For users of my analysis site: https://microbiomeprescription.com/, for diagnostic purposes there are few differences! We have general agreement for:
End Product Production
Medical Studies Matches
Symptom Matches
Detecting high or low levels by percentile
The critical difference between the information lab providers and my site is interpretation sophistication.
So, to answer the reader’s question “The numbers are in major disagreement, but the diagnostic significance of the whole sample is in strong agreement”. Doing the lab analysis is worth it — just ignore the lab’s “value added” suggestions/information.
Rosefrom BiomeSight and Richard from Thryve are both invited to submit a blog post (send to me as a Word Document) to get their thoughts and analysis shared.
Challenge to the same two people: Take one stool, do 100 samples from it and process them all. Make the data public — or get an academic to write an article on the consistency (or inconsistency) of data from a single sample. How many distinct samples are needed to get convergence of numbers (and how much convergence). The numbers will vary according to lab equipment and process.
“Alterations of the gut microbiome in anorexianervosa have been demonstrated, but their clinical relevance remains unclear. ” [2020]
“We have recently reported specific fecal metabolomic changes in acute and short-term weight restored patients with anorexianervosa (AN). In this study we explored the association between those metabolomic changes and patients’ gut microbiome” [2020]
The Microbiome is only a Part — but the easiest to modify
For almost all of the above conditions there are known DNA mutations associated (SNPs). We know that there is an interaction between the DNA and the microbiome — effectively the microbiome is an organ. Organs have compatibility issues when transplanted. A similar failure to take has been observed with Fecal Matter Transplant.
The simplest model to understand what is happening is this: the DNA favors bacteria that favors the DNA desired behavior (be it good or bad). Basic self-serving “microbiome forming” by the DNA. Over time, the DNA may alter its behavior due to environmental factors like stress (epigenetics) and in a few cases, RNA from a virus may be taken up into the DNA. In reality, it is estimated that up to 50% of your DNA originated from a virus [Src 2020]… ongoing incorporation of new virus fragments remains a possibility.
The question is how do you stop the undesirable behavior? You could attempt to alter the DNA — that is very experimental with considerable risk. You could use drugs that appear to inhibit the undesirable behavior — drugs tried at random on a population in a study with positive results. Often we do not know the mechanism of the drug — simply that they worked.
My more unconventional approach is to “strong arm” the bacteria. Yes, DNA is encouraging one pattern — but with food, diet, supplements it appears possible to alter the pattern. I have seen my own SPECT scan go from appearing to be early Alzheimer’s disease back to normal by this method.
Is 100% recovery expected — no, improvement is expected. Often very significant improvement. Is there actual evidence? FMT or Fecal Matter Transplant is the clearest demonstration… you change the gut bacteria and see if there are changes!
Clinical trials with FMT have been performed in patients with autism spectrum disorder and showed beneficial effects on neurological symptoms. For multiple sclerosis and Parkinson’s disease, several animal studies suggested a positive effect of FMT, supported by some human case reports. For epilepsy, Tourette syndrome, and diabetic neuropathy some studies suggested a beneficial effect of FMT, but evidence was restricted to case reports and limited numbers of animal studies. For stroke, Alzheimer’s disease and Guillain-Barré syndrome only studies with animal models were identified. These studies suggested a potential beneficial effect of healthy donor FMT. … Whether positive findings from animal studies can be confirmed in the treatment of human diseases awaits to be seen. Several trials with FMT as treatment for the above mentioned neurological disorders are planned or ongoing, as well as for amyotrophic lateral sclerosis.
Viral re-activation is common with ME/CFS [2017]. It’s a chicken and the egg scenario. Did the viral re-activation cause ME/CFS or did ME/CFS cause viral re-activation. Most people do not ask about the third leg of this stool: Was there something else that contributed to both viral re-activation and ME/CFS (or the contemporary “Long Haul Covid” syndrome).
My model for ME/CFS is a microbiome dysfunction. So the question becomes, can a microbiome dysfunction also account for viral re-activation? Latest research says yes and identifies some bacteria involved!
Correlation analyses between the microbiome and viral titers revealed a positive correlation with Gracilibacteria, Absconditabacteria, and Abiotrophia and a negative correlation between Oribacterium, Veillonella, and Haemophilus. There was also a significant positive correlation between microbiome richness and EBV viral titers.
It appears to be a two way street: “Our study is the first to report the impact of long-term subclinical CMV infection on host immunity and gut microbiota” [2018]
It also extends to the food that is consumed and microbiome interaction (i.e. production of short- and medium-chain fatty acids by some bacteria consuming the food).
Our studies of the differential activities of SCFAs and MCFAs as inducers or inhibitors of viral reactivation have implications for oncolytic strategies. The HDAC inhibitors butyrate, phenylbutyrate, and VPA have been investigated as lytic activators in cells, mice, and patients (31, 85,–89). One risk of applying lytic induction therapy is that incomplete inhibition of viral replication by antiviral drugs could allow secondary infection and disease progression
Vitamin D levels are usually low, very low with ME/CFS patients. “vitamin D deficiency can be considered as a risk factor for CMV reactivation”[2019] “For EBV, viral load was significantly higher when 25(OH)D levels were low, demonstrating an inverse correlation between 25(OH)D levels and EBV load. ” [2018]. Anna Dorothea Hoeck,MD, has had success in putting some ME/CFS patients in remission by using high dosages of Vitamin D (likely those that also has viral reactivation).
Bottom Line
While there is not an abundance of literature, we see that the metabolites produced by the microbiome can activate or deactivate existing latent viral infections. We also know a shift in bacteria is associated with increase viral titers. Last, we know that virus can alter the microbiome.
We end up with three legs on the stool with the microbiome being significant. It is very significant because it is the easiest to change.
Virus reactivation alters the microbiome which then produces metabolites causing fatigue, etc. The altered microbiome then feeds the virus…. I have often used the expression “Viro-forming the microbiome”. It’s a feedback loop that can be hard to break.
A reader from Europe has ME/CFS with severe brain fog. One of the challenges with Microbiome manipulations is that there are many, many approaches that may be taken. We do not have clear evidence on which has better results. Rather than prescribing a magic bullet path, I have made most of these paths available on Microbiome Prescription.
For the brain fog, this presents a dilemma. I have Dr. Jason Hawrelak’s recommendations for quick, ultra-generalized suggestions. In corresponding with this reader, I realized that the loss of executive decision making and brain fog — very common with ME/CFS (and I have experienced it) — left the person as the typical “deer in headlights’ seen with ME/CFS.
This week, I came up with a elegant solution. Using the microbiome sample and the symptoms that have been entered, I crafted some AI to generate suggestions based on the strong statistical relationships we have discovered via citizen science. Preliminary results are looking good.
To use this, you must enter your symptoms when the sample was taken. It uses both the sample and the declared symptoms.
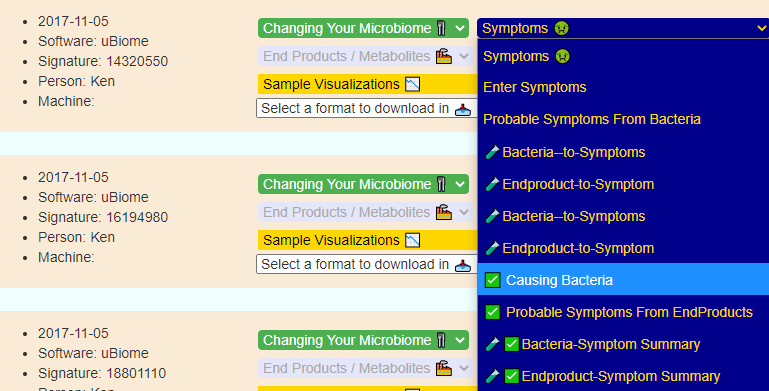
This feature is under Symptoms / Causing Bacteria
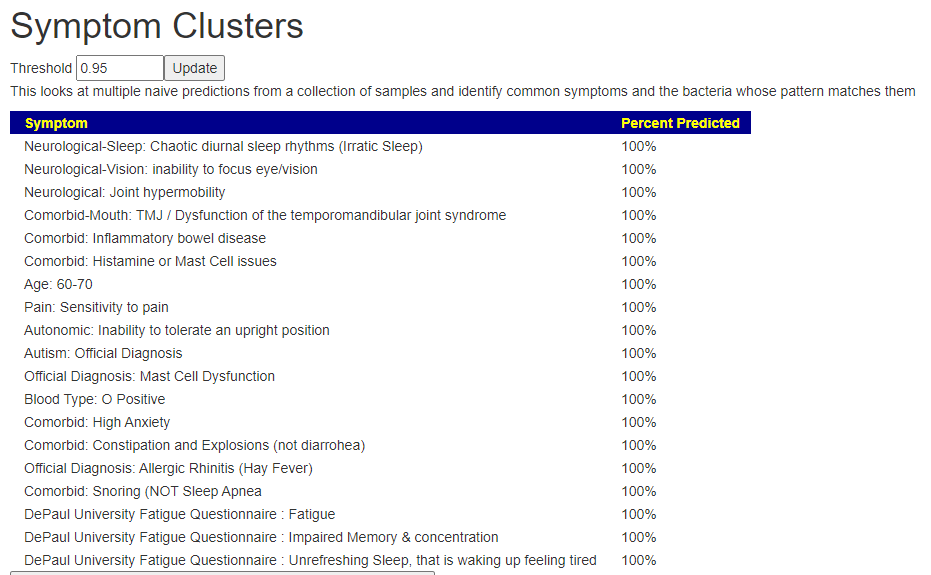
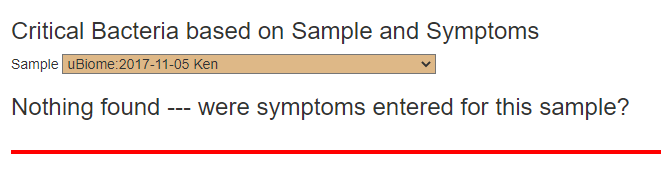
If you do not have any symptoms entered (or the symptoms lacks strong associations with the current data), you will see this display
Check the symptoms for the sample — do you have all of them?
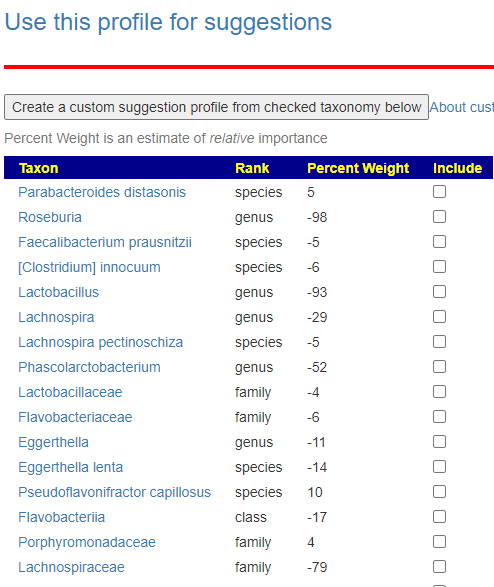
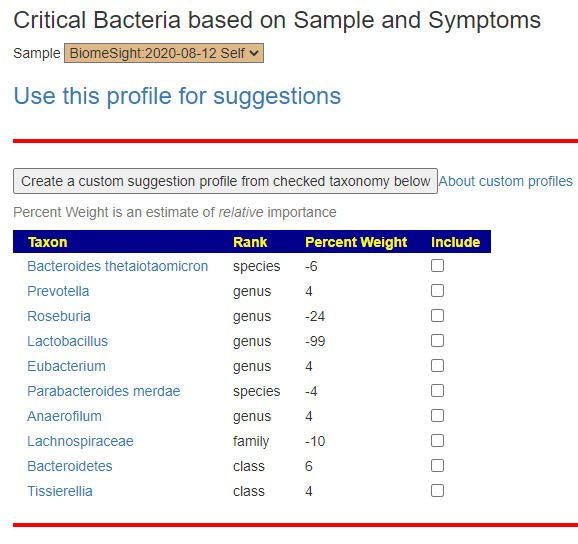
Your results may look like this:
Ken’s result during a ME/CFS relapse. Negative means too few. Positive means too many
This reader’s list is much shorted, but with several things in common
You have two choices on getting suggestions…. Clicking the “use this profile for suggestions” OR build out a custom profile. If you are brain-fogged… do the first.
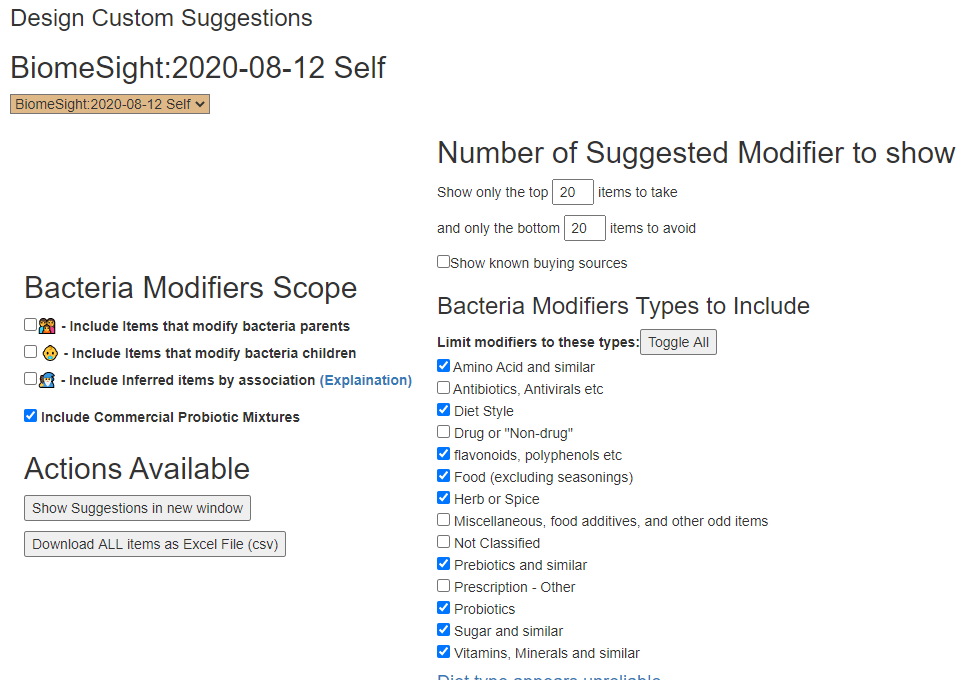
This takes you to the usual suggestion page where you can scope suggestions.
If you are brain-fog, leave as is, or uncheck some items
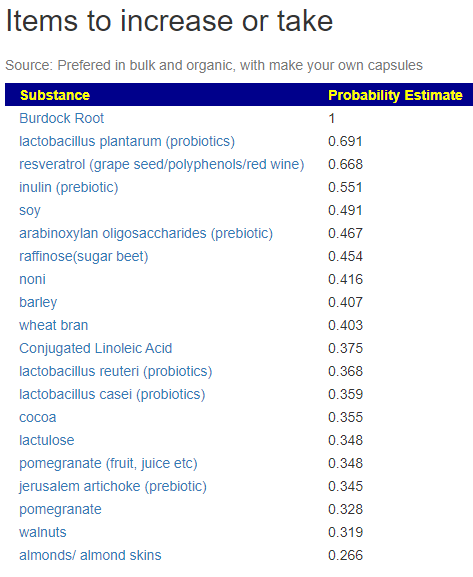
This then takes you to the suggestions page.
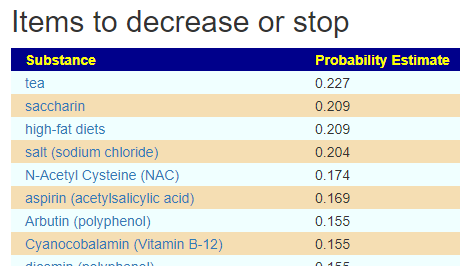
For this reader, all of his avoids had less weight than most of the items above… so it is mainly a take this result.
The values in this case are so low, that you can reasonably ignore them
And the list goes on with Apples, magnesium, selenium, oregano being on the positive list by inference.
Feed Back from the EU Reader
“Thank you very much for your help you can use in the future my data to write blog posts if you want no problem. You made me cry of joy in a dark hour. Interesting return of result so the Jadin Model fits me:”
I used the Jadin antibiotics (following her rotation protocol) with great success in one of mine earlier relapses. He has a cooperative MD that is willing to prescribe them. Rifaximin became available after that protocol became available – it has been cited on several ME/CFS sites [1] [2]. Personally, I would keep to the Jadin protocol and only include if after a couple of cycles there has not been sufficient progress.
As a FYI: I am pleasantly delighted that the antibiotics predictions came out matching Jadin’s protocol and isolated a small number of high value antibiotics to consider.