Both of the people below used the model to make major progress on CFS. When you read their accounts you may be a little shocked by the difference of what they did. There is no “step-by-step magical protocol”, you have to work with what you can get and note your response to things, keep changing until you find the effective combination.
Both of these readers used earth based organism probiotics (i.e. what your ancestors would have been gotten walking through the fields chewing a stalk of grass or other grain (unwashed) in your mouth): Prescript Assist or Equilibrium. Without knowing it, they were taking probiotics in a natural form. Of course, today most fields are rich is pesticides and such, so chewing grass is not advised.
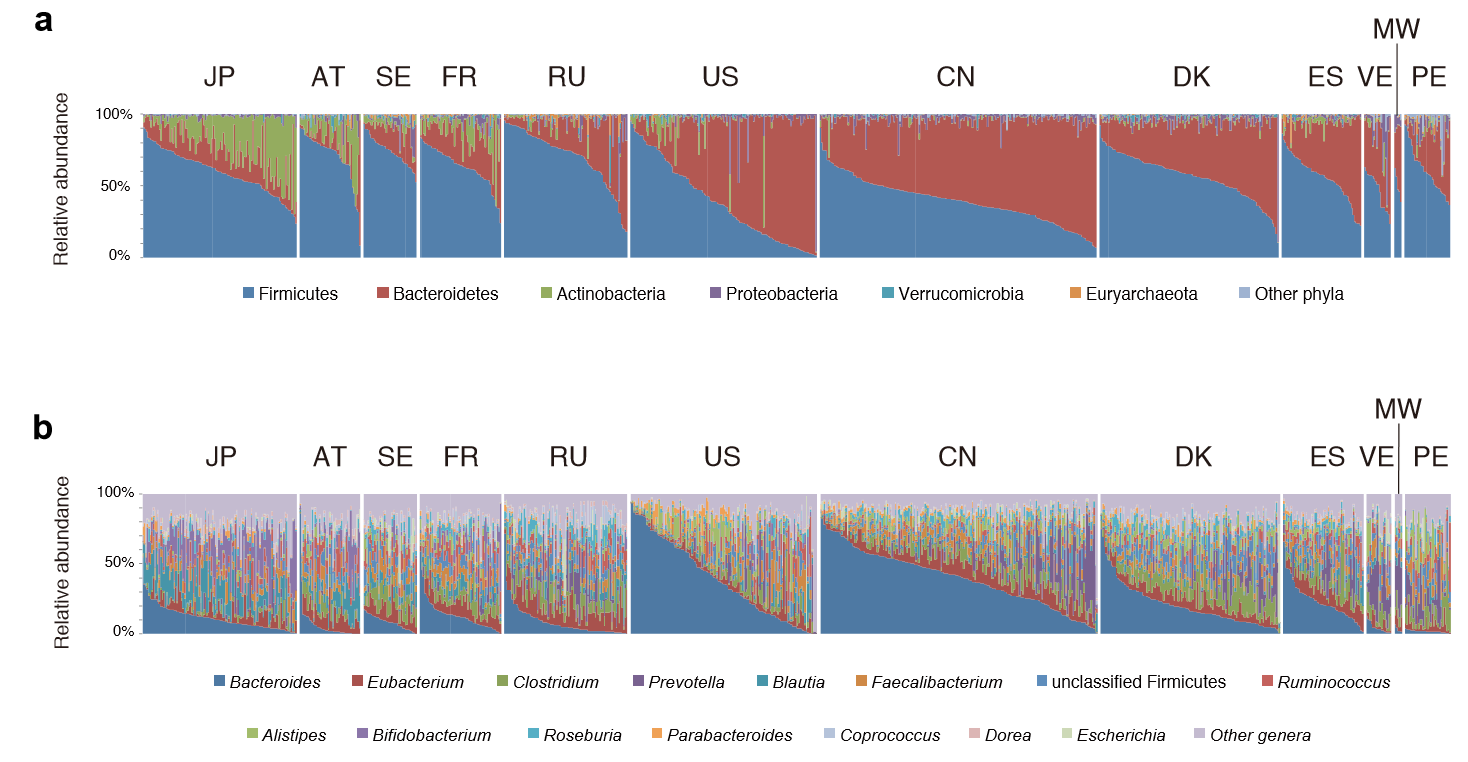
There are differences in agricultural practices between two very similar genetic and diet groups. “asthma prevalence is 2–3% among the Amish, who practice traditional farming, and 15% or higher among the Hutterites, who embrace modern farming.”
I suspect two factors: one is residue pesticide levels on the fields (yes, Hutterites use pesticides!); the second factor is that I suspect difference of attitudes to chewing on a stalk of wheat by kids (“No harm, I did it too!” vs “It may have pesticides on it, take it out of your mouth!”)
The very Simple Remission
This case deals with someone that the right probiotic for them happen to trigger the cascade for remission.
“Thank you SO much for your blog! I recently asked you a question on your blog – I am the gal w IBS based ME CFS who partially recovered (was down to 25-30% of activity, bed/housebound w severe PEM, recovered to about 65-70%), and entirely by chance, taking VSL#3 (I hadn’t discovered your website yet). I switched over to Prescript Assist, and it hasn’t even been a week yet, and yesterday, for the first time in 6 months I went for a 2 mile walk/jog around my neighborhood. My mono symptoms have disappeared. I have an appt. w Dr. xxx in 2 weeks, which I’m going to keep, but my recovery is something I never could have imagined! I never would have found Prescript Assist if it wasn’t for your blog and I just can’t thank you enough…it was a Godsend! I have my life back – I will be able to attend both my sons’ graduations and take my elder son to college in the Fall, which I never imagined I’d be able to do…”
The Hard Fought Remission
This person fought for remission by herbs, probiotics and antibiotics.
“BTW – I’m working full time now!
After a few years of essentially being too weak to leave house or even blog, this is a huge breakthrough for me. I hope I can stay as high-functioning as I am now. Still a bit unsure which intervention pushed me over the edge of functional but very grateful for you and your site. Thank you Ken!
For instance, I likely would have resisted chronic antibiotic use if I hadn’t read your site. And I had given up on going to doctors (although now that I have a job again, I have an appointment with a new integrative doctor 5/22). Antibiotics are definitely the foundation of my recovery. If I had to estimate, I’d assign various treatments this rough spread of credit:
Pretty simple model. Doxy kills bad bacteria. Kapsida also works as antimicrobial and seems to potentiate other antibiotics. Bursts of Equalibrium and Mutaflor definitely add baseline wellbeing and energy over antibiotics alone.
Rapamycin resets immune system whenever antibiotics stop working. Amazing to bounce back same day vs random downward tolerance spirals where everything stops working.
LDN serves same function as Rapamycin. It can additionally reset any stimulant tolerance. I try not to take high enough doses of stimulants to develop tolerance there too often so I mostly skip LDN unless I’m really in trouble. It’s definitely the ickiest drug in my mix and probably net bad for anyone long-term.
Armodafinil obviously extends willpower, mood, and vigilance. It’s a band-aid but even half doses are a really good bandaid. It takes me from simply well enough to sit up on the coach and not feel weak –> well-enough to work in an office with others all day.
Don’t really know/understand yet why Mt Dew is only caffeine source that seems beneficial. I’m starting to wonder if caffeine is not what I’m enjoying about Mt Dew. I really don’t get any positive mental effects from coffee or tea or any other soda. Also, even slight variants of Mtn Dew don’t work (like Diet Mt Dew or Mt Dew: White Out). Very strange. I was just looking thru ingredients list as I was writing this to you:
- Mtn Dew throwback w/ sugar (works)
- Mtn Dew: Code White (doesn’t work?!?)
- Diet Mtn Dew (doesn’t work!?)
Hmm. This set is actually enough to identify the compound in Mtn Dew that apparently benefiting me:
That seems ridiculous.
Anyway, thanks again for sharing all your research on cfsremission.com. Let me know if there’s ever any way I can help you out. I’d be unemployed, laying on my gf’s couch (hard to pay rent w/ cfs) trying to muster the energy to play PS4 games right now if it weren’t for you.”
Erythorbic acid
NOTE: This does not appear to be in all Mountain Dew. Formula differs from country to country. In Europe,
Erythorbic acid is known as E-315. It is not in Spanish Mountain Dew.
Others names for Erythorbic acid are:
- D-araboascorbic acid
- erythorbic acid
- erythroascorbic acid
- isoascorbic acid
- isoascorbic acid, disodium salt
- isoascorbic acid, monosodium salt
- isoascorbic acid, sodium salt
- sodium erythorbate
Same citation provided the following information also:
- Erythorbic acid is readily absorbed and metabolized. Following an oral dose of 500 mg of erythorbic acid to human subjects the blood level curves for ascorbic acid and erythorbic acid showed a similar rise. In five human subjects, an oral dose of 300 mg was shown to have no effect on urinary excretion of ascorbic acid. http://www.inchem.org/documents/jecfa/jecmono/v28je03.htm
- These results indicated that the gastrointestinal permeability differed between the two chemicals.
- In dogs, this resulted in a half-life of approximately 30 minutes for erythorbic acid in the plasma.
- “The thermal inactivation of Salmonella thompson, Escherichia coli, Staphylococcus aureus, Clostridium perfringens, Candida zeylanoides, Enterococcus faecium and E. faecalis was accelerated by the addition of sodium isoascorbate (1 mmol/l) to phosphate-buffer heating medium but not to complex food mixtures.” [1989]
- Erythorbic acid is a potent enhancer of nonheme-iron absorption [2004]. “Iron absorption from the test meal without any added enhancer was 4.1%. The addition of erythorbic acid (at molar ratios of 2:1 and 4:1 relative to iron) increased iron absorption 2.6-fold (10.8%; P < 0.0001) and 4.6-fold (18.8%; P < 0.0001), respectively.”
Bottom Line for Erythorbic acid
It appears to be very safe and appears effective against some food bacteria (used as food preservative to preserve food better). It is recognized as an antioxidant. It appears to assist in some fighting of bacteria.
We do not have enough information to recommend or not. We know that it impacts bacteria. We know that it seems to make a significant difference for on CFS sufferer.
The dosage in a bottle of Mountain Dew is likely low, and 500 mg dosages have been tested on humans with no adverse effects. This suggests for more adventuresome readers, that a dosage of 100-500 mg/day be tried (if you do try, please post results — or no results — on this post).
It is available as a powder, in Spain, some manufacturers listed here