A CFS reader wrote with some really tough questions concerning their infant….
“This week, I’m off on another tangent – gluten intolerance, especially in babies. My daughter turns 6 months old in 2 weeks time and I’m ready to start introducing solids. The problem I have is that the latest information is so conflicting. (Note: these studies have only been done specifically on Celiac Disease). “
“Thoughts that I have in my head are:
- I am gluten sensitive with CFS and this is linked to my gut microbiota;
- My baby inherited my gut microbiota when she was born;
- Has she inherited all of my newly introduced probiotics via breastfeeding since she was born?
- Being a parent is so much pressure!!! I have this little girl’s lifelong health in my hands!!!
I’ve been reading up on your info on gluten and learned that Bifidobacteria play a role in gluten allergies”
“So, I guess my question is –
When I introduce gluten into my daughter’s diet, do you think that supplementing her with multiple Bifidobacteria strains will help her digestive transition and help her to avoid sensitivity to gluten?”
The Research
- “this research observed that E. coli releases uracil. L. plantarum specifically recognizes E. coli-derived uracil, which increases the growth rate and production of antimicrobial substance of L. plantarum. In addition, through the inhibitory activity test, this study postulates that the antimicrobial substance is a protein and can be considered a bacteriocin-like substance. Therefore, this research assumes that L. plantarum exerts its antibacterial ability by recognizing E. coli and increasing its growth rate as a result, and this phenomenon could be one of the reasons for L. plantarum settling in the intestine of infants as a beneficial bacterium.” [2016]
- ” the supplementation with Lactobacillus rhamnosus GG has been associated with the development of sepsis with a cause-effect relationship in six newborns and children. In this study, we report two further cases and discuss the emerging issue of probiotic supplementation safety in neonates. We conclude that physicians must be aware that supplementation with L. rhamnosus GG can cause sepsis in high-risk patients on rare occasions.” [2016]
- “Effects have been most consistent with combined prenatal and direct postnatal supplementation of the infant and appear strain-specific, with Lactobacillus rhamnosus most often showing an effect.” [2013]
- “Among the twelve Bifidobacterium sp. strains, the largest spectrum of antimicrobial activity against 9 of the 18 enteropathogenic strains was revealed for a B. breve strain recently isolated from infant intestinal feces.” [2016]
- ” In a recent meta-analysis, the use of multi-strain probiotics appeared to be most effective for eczema prevention.” [2016]
- “Predictors for any food hypersensitivity were wheeze, maternal atopy, increasing gestational age, age at first solid food introduction and mean healthy dietary pattern score. Predictors for IgE mediated allergy were eczema, rhinitis and healthy dietary pattern score whereas for non-IgE-mediated food allergy the predictors were dog in the home, healthy dietary pattern score, maternal consumption of probiotics during breastfeeding and age at first solid food introduction .” [2016 – full article]
- Increased risk: OLDER age at first solids and concurrent breastfeeding with cows’ milk from any source.
- “There is evidence that the addition of prebiotics to infant formula brings the GI microbiota of formula-fed infants closer to that of breast-fed infants.” [2015]
- “we gave Bifidobacterium breve M-16V and Bifidobacterium longum BB536 prenatally to 130 mothers beginning 1 month prior to delivery and postnatally to their infants for 6 months….These data suggest that the prenatal and postnatal supplementation of bifidobacteria is effective in primary preventing allergic diseases. Some limited changes in the composition of fecal microbiota by the bifidobacterial supplementation were observed.” [2014]
- “the probiotic (Lactobacillus salivarius CUL61, Lactobacillus paracasei CUL08, Bifidobacterium animalis subspecies lactis CUL34 and Bifidobacterium bifidum CUL20;) … seemed to prevent atopic sensitisation to common food allergens”
Microbiome
- “Alterations in specific bacterial groups metabolising gluten such as Clostridium or Lactobacillus were reported in Coeliac disease (CD) patients. ” [2015]
- “The treated CD patients showed a reduction in the diversity of Lactobacillus and Bifidobacterium species. The presence of Bifidobacterium bifidum was significantly higher in untreated CD patients than healthy adults.” [2012]
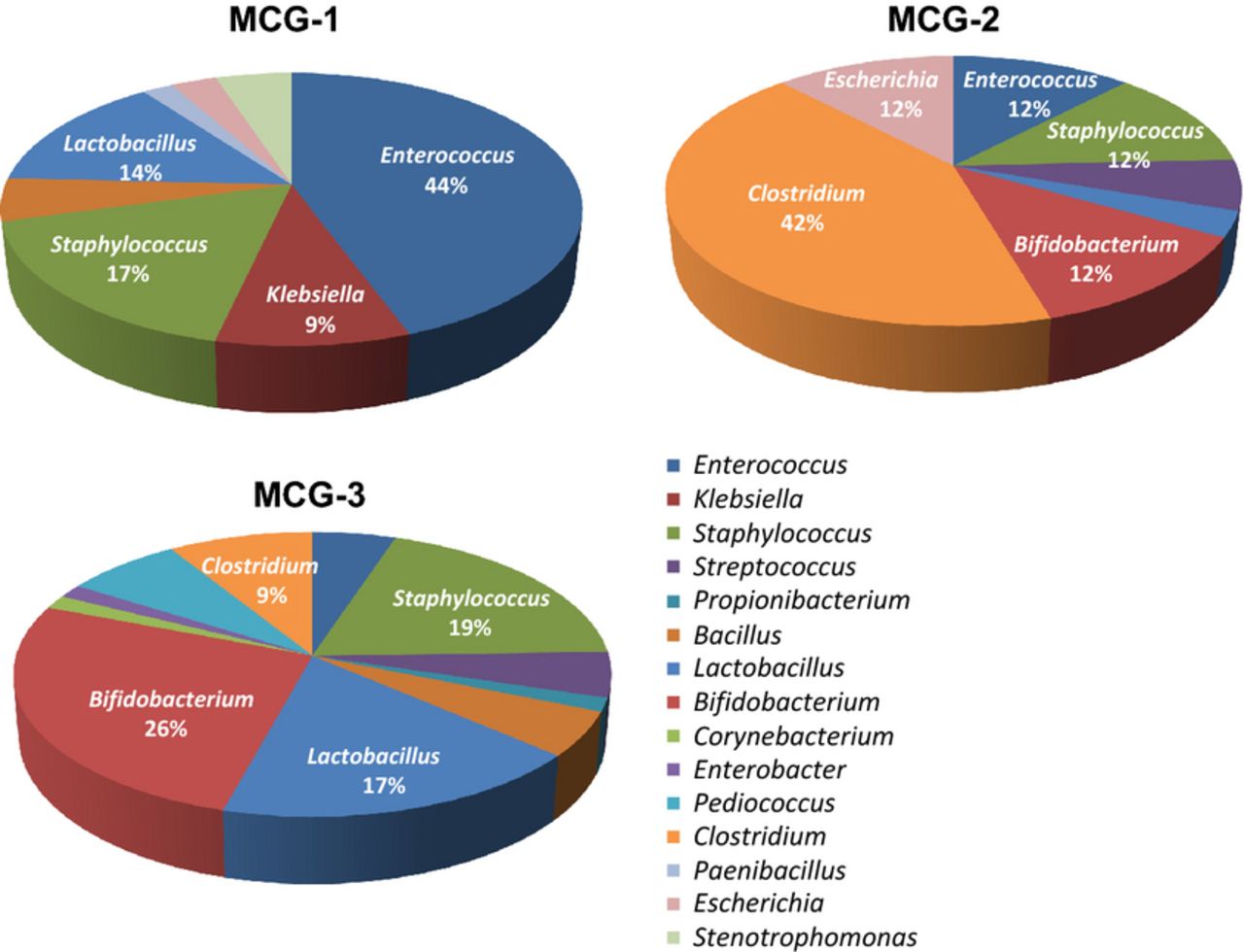
- “Bacteria involved in gluten metabolism are mainly Firmicutes and Actinobacteria” [2014 a deep dive study – the chart below is from it]

- “We isolated 144 strains belonging to 35 bacterial species that could be involved in gluten metabolism in the human gut (Table ⇑). Most of the strains were classified within the phylum Firmicutes (c. 73%), mainly from the genera Lactobacillus, Streptococcus, Staphylococcus and Clostridium. Some 15% of the isolates were classified within the phylum Actinobacteria, mostly from the genus Bifidobacterium. Only 12% of the isolates were Gram-negative bacteria from the phylum Proteobacteria.”
- “61 of these 144 strains showed an extracellular proteolytic activity against gluten proteins and gelatine. This glutenasic activity was present in strains from Bacillus licheniformis, B. subtilis, B. pumilus, Bifidobacterium longum, Clostridium sordellii, C. perfringens, C. botulinum/sporogenes, C. butyricum/beijerinckii, Enterococcus faecalis, E. faecium, Propionibacterium acnes, Pediococcus acidilactici, Paenibacillus jamilae, Staphylococcus epidermidis, S. hominis and Stenotrophomonas maltophilia.”
- “Although bacterial strains belonging to Enterococcus faecalis or Bacillus licheniformisexhibited activity, the peptide was not completely hydrolysed. In contrast, other bacteria, such asLactobacillus mucosae (strains B1c and D5a1), L. rhamnosus (strains LA2a, LE3 and D1a) andClostridium botulinum/sporogenes (all isolated strains) appeared to have a higher activity with regard to the 33-mer peptide than other bacteria tested”
- “However, not all the bacteria involved in gluten metabolism are health promoting. Bacterial proteases of certain groups isolated in this work, including Staphylococcus epidermidis, Enterococcus faecalis,Escherichia coli, Clostridium perfringens and C. sordellii, may be related to inflammatory bowel disease (Pruteanu et al., 2011; Steck et al., 2012).”
- “We are currently studying whether these bacteria have a protecting and/or a pathogenic role in CD.”
- Lower bifidobacteria counts in adult patients with celiac disease on a gluten-free diet [2014].
- “That study found that the probiotic VSL#3 was highly effective in hydrolyzing gliadin polypeptides compared to other commercial probiotic products such as Oxadrop (B. infantis, L. acidophilus, L. brevis, and S. thermophilus), Florisia (L. brevis, L. salivarius subsp. salicinius, and L. plantarum), and Yovis (B. breve, B. infantis, B. longum, L. acidophilus, L. plantarum, L. casei, L. delbrueckii subsp. bulgaricus, Streptococcus salivarius subsp. thermophilus, and Enterococcus faecium).” [2014]
- “Higher Bacteroides counts are detected in CD children (13, 26) than in controls.”
- “Data on the levels of Atopobium, Staphylococcus, E. coli, Eubacterium rectale–C. coccoides, the Clostridium histolyticum group, Clostridium lituseburense, and sulfate-reducing bacteria are still contradictory, as there have been reports showing increased levels in CD patients (13) or no difference (26, 28, 30) in comparison to controls.”
- “The ratio of beneficial lactobacilli and bifidobacteria to possibly harmful Gram-negative bacteria, such as Bacteroides-Prevotella and E. coli, was found to be significantly higher in controls than in CD children (26). It has been shown that levels of specific species of lactobacilli and bifidobacteria may be higher, lower, or not detected in CD patients in comparison to controls (). However, the exact value of this information still remains unclear.”
Best attempt to answer…
- Has she inherited all of my newly introduced probiotics via breastfeeding since she was born?
- “Probiotic bacteria administered to mothers during late gestation are transferred to infants born vaginally and influence the assemblages of GIT bacteria. However, colonization of the neonatal GIT and persistence past weaning does not occur in all offspring and varies among probiotics and animal models.” [2010]
- “Temporary colonization of an infant with L. GG may be possible by colonizing the pregnant mother before delivery. Colonization is stable for as long as 6 months, and in unexplained circumstances may persist for as long as 24 months.” [2004]
- “Alterations of the maternal GIT microbiota composition via supplementation with probiotics and prebiotics have been shown; however, transfer of these benefits to the offspring remains to be demonstrated.” [2012] [Full Text]
- “experiments with pregnant mice orally administered a labeled Enterococcus faecium strain showed a low level transfer of the labeled strain to the fetal intestine and a higher level transfer to the mammary glands”
- “the maternal immune status seems to affect infant GIT microbiota composition as well as the incidence of allergic diseases. Allergic mothers, e.g., had lower amounts of bifidobacteria in their breast milk and feces and, consequently, decreased counts and diversity of bifidobacteria in the offspring feces (74, 75) compared with nonallergic mothers. The establishment of specific microbiota in infants, such as bifidobacteria (76), has been shown to alter the signaling reactions that determine T-cell differentiation and/or the induction of tolerance (77, 78).”
Recommendations To Discuss with Your Medical Professional
It appears that the issue is with Bifidobacteria — but at the species or strain level. That is, some are good and some are bad. See [2014] for a lot of detail in Table 1, including citing explicit strains that appear to be helpful. Of course, the problem is finding these strains commercially.
- L. plantarum
- Bifidobacterium Breve, see also [2015]
- Bifidobacterium longum BB536
- No Bifidobacterium bifidum
- NO L. rhamnosus GG – because multiple adverse results have been reported.
While neither Prescript Assist nor General Biotics’s equilibrium were cited – they may qualify under multi-strain probiotics.
A dutch page on gluten cites Symbioflor-1 (Enterococcus faecalis )for glutten (page) without giving references. There is one possible articles supporting this:
- “The combined use of enterococci and fungal proteases showed a decrease of the gluten concentration of more than 98% during long-time fermentation.” [2009]
No Prepared Foods
- “Unfortunately, gluten has proven to be toxic for a proportion of people that in the last few decades has been constantly rising (Rubio-Tapia et al., 2009). Indeed, the wheat varieties that contain the most detrimental type of gluten have become more common (van den Broeck et al., 2010). This is particularly worrying given that gluten is not only naturally present in bread, cake, pasta, pizza, and beer, but it is—for its binding and thickening properties—also added to an impressive variety of other products. A survey of Australian supermarkets found gluten in nearly 2,000 different food items, ranging from sauces to processed meats, and over 100 non-foods, from pain relievers to shampoos (Atchison et al., 2010). Yet gluten triggers some action as soon as it turns up in the gut—not only in a few sensitive people, but in all of us.” [2016] – Thus avoid all prepared foods, especially baby foods…. made from scratch may be the best path.
Summary of Bacteria Shifts
The results are not consistent across studies. The table below show the shift reported. Some items are in both list. My general conclusion is that general lactobacillus probiotics should be avoided, but a few select one are suggested.
The increase of diversity suggests that evil strains of lactobacillus and bifidobacteria have populated. These strains may be evil solely because they do not process gluten.
| With Glutten /Celiac Issues |
|
| Increase |
Decrease |
| Bacteroides |
Akkermansia muciniphila |
| Actinobacteria |
Bacteroides-Prevotella |
| Atopobium |
Bifidobacterium |
| bacterial diversity |
Bifidobacterium adolescentis |
| Bacteroides-Prevotella |
Bifidobacterium bifidum |
| Bifidobacterium |
Bifidobacterium catenulatum |
| Bifidobacterium adolescentis |
Bifidobacterium lactis |
| Bifidobacterium Bifidum |
Bifidobacterium diversity |
| Bifidobacterium breve |
Clostridium coccoides |
| Bifidobacterium dentium |
Deinicoccus-Thermus |
| Clostridium |
Haemophilus spp. |
| Clostridium histolyticum |
Lactobacillus casei |
| Clostridium lituseburense |
Lactobacillus paracasei |
| Enterococcus, |
Lactobacillus Rhamnosus |
| Escherichia coli |
Lactobacillus sakei |
| Eubacterium rectale-Clostridium coccoides |
Lactobacillus zeae |
| Faecalibacterium prausnitzii |
Lactobacillus |
| Firmicutes |
Lactobacillus-Bifidobacterium/Bacteroides-Prevotellaratio RATIO |
| Fusobacteria |
Neisseria spp. |
| Lactobacillus |
Porphyromonas |
| Lactobacillus Brevis |
Proteobacteria |
| Lactobacillus curvatus |
Proteobacteria |
| Lactobacillus delbrueckii bulgaricus |
Staphylococcus |
| Lactobacillus frementum |
Staphylococcus-Micrococcus |
| Lactobacillus gasseri |
|
| Lactobacillus paracasei |
|
| Lactobacillus plantarium |
|
| Lactobacillus Rhamnosus |
|
| Lactobacillus Rossiae |
|
| Lactobacillus and Bifidobacterium groups greater diversity |
| Leuconostoc carnosum |
|
| Leuconostoc mesenteroides |
|
| Methylobacterium spp. |
|
| Mycobacterium spp. |
|
| Staphylococcus |
|
| sulfate-reducing bacteria |
|