A reader forwarded a new study from March, 2021. Unfortunately, ME/CFS seems to be in an infinite loop of similar hypotheses that keep repeating with a preliminary investigation and recommendations that are not followed up. I have seen this pattern over the decades that I have followed CFS/ME research.
Potential role of microbiome in Chronic Fatigue Syndrome/Myalgic Encephalomyelits (CFS/ME)
The present research explored the composition of the intestinal and oral microbiota in CFS/ME patients as compared to healthy controls. The fecal metabolomic profile of a subgroup of CFS/ME patients was also compared with the one of healthy controls. The fecal and salivary bacterial composition in CFS/ME patients was investigated by Illumina sequencing of 16S rRNA gene amplicons. The metabolomic analysis was performed by an UHPLC-MS. The fecal microbiota of CFS/ME patients showed a reduction of Lachnospiraceae, particularly Anaerostipes, and an increased abundance of genera Bacteroides and Phascolarctobacterium compared to the non-CFS/ME groups. The oral microbiota of CFS/ME patients showed an increase of Rothia dentocariosa. The fecal metabolomic profile of CFS/ME patients revealed high levels of glutamic acid and argininosuccinic acid, together with a decrease of alpha-tocopherol. Our results reveal microbial signatures of dysbiosis in the intestinal microbiota of CFS/ME patients. Further studies are needed to better understand if the microbial composition changes are cause or consequence of the onset of CFS/ME and if they are related to any of the several secondary symptoms.
Abstract
This is not a new finding. Similar have been reported — dating back to 1998. For prior studies see these links:
- PubMed Conditions Citations for Chronic Fatigue Syndrome
- PubMed Conditions Citations for ME/CFS with IBS
- PubMed Conditions Citations for ME/CFS without IBS
Going thru the article and the methodology, I was disappointed on the use of ancient data-analysis (Principal Component Analysis, Canonical correspondence analysis) instead of Random Forest. Moving over to the good news.
The Microbiome of the ME/CFS mouth is a factor!
The study illustrated a clear pattern between controls, patients and the patients’ relatives
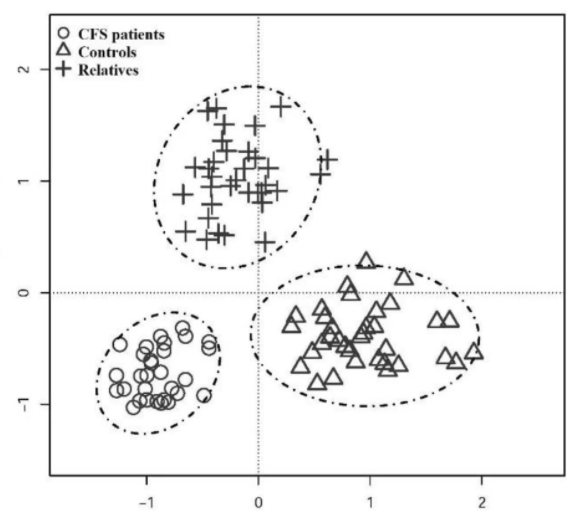
This suggests that there is a pre-disposition via the salivary microbiome for ME/CFS. The salivary microbiome is formed by kisses, and just being in the same living space (this was demonstrated in a recent study where the microbiome of family pets were transferred to the children [2021] [2021])
It is nice to see this clearly demonstrated. This has been reported prior Chronic fatigue syndrome patients have alterations in their oral microbiome composition and function. [Sep 2018]
In prior posts, over the last 7 years, I have flagged this issue:
- A mouth full – for better or worst [2014]
- Your mouth can trigger flares [2017]
- Science based mouth wash for ME/CFS [2019]
What are the changes in the mouth bacteria (with links to what modifies these bacteria)
- Actinobacteria (High)
- Actinomycetales (High)
- Micrococcaceae (High)
- Rothia (High)
Bottom Line
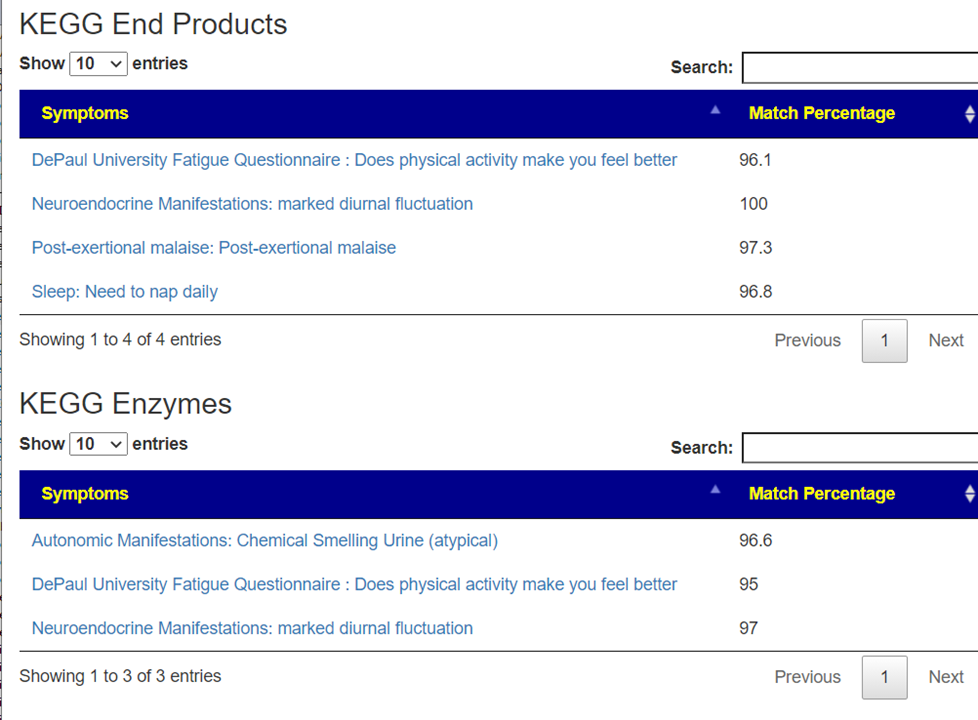
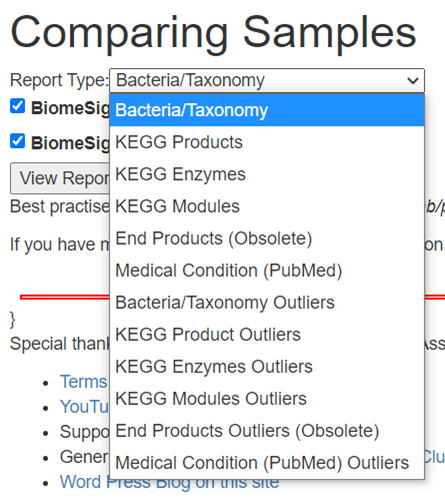
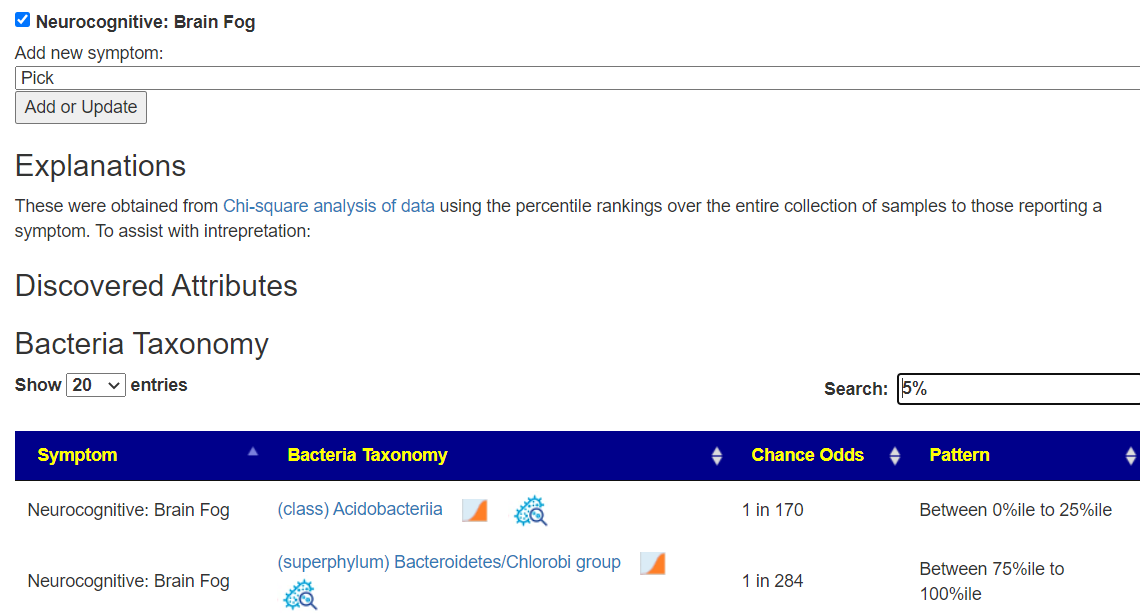
The authors asked “if they are related to any of the several secondary symptoms“, the answer is yes. For several years we have demonstrated that on Microbiome Prescription with citizen science.
Similarly, “if the microbial composition changes are cause or consequence of the onset of CFS/ME” can be answered as: Some transitory event (i.e. infection, stress, vaccination) causes a change of the microbiome composition. This altered composition takes on a life of its own and cascade into ME/CFS.
My own experience, and some others, are that by altering the microbiome composition back towards normal, ME/CFS improves or disappears.
The unfortunate aspect is that it cannot be handled in ‘one drug solves it’ or a pro-forma cookbook by medical professionals. Every individual has a different microbiome shift with items suggested for one ME/CFS person being contraindicated for a different ME/CFS person based on their 16s determined microbiome and using the artificial intelligence used for suggestions on Microbiome Prescription.
My expectations are that they will be no traction towards treating ME/CFS by conventional researchers. The reason is simple — the ground rules for studies and processes will send them into cascading challenges which required “stepping outside” of establish processes to get traction. This has been described as the “Dogma of Conformity”.