A reader asked:
“Do you still think thick blood is a common issue and do you still recommend getting the multiple labs for thick blood? Is there a viscosity test you recommend for seeing that the thickness is at any given time?”
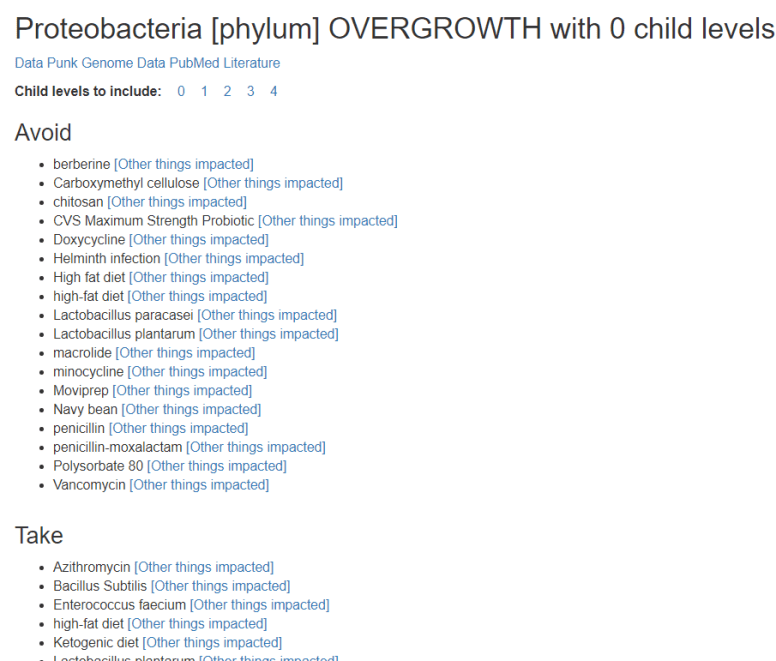
Given that I have been focusing on the microbiome (mainly because it is actionable in many ways — diet, probiotics, antibiotics; and easily measurable => ubiome.com), it is a good question to ask and to remind people that this can be a significant factor and it is not isolated from the microbiome!
Literature
“Many bacteria and bacterial components can directly activate individual human coagulation factors. However, direct initiation of the coagulation cascade and the formation of a propagating clot are not typically observed11–17. These bacterial components usually activate low levels of coagulation factors, which does not result in the amplification and positive feedback necessary to form a clot that can grow and propagate. For example, Staphylococcus aureus produces coagulase, a protein that binds prothrombin stoichiometrically and leads to cleavage of fibrinogen to fibrin14. However, this conversion simply precipitates fibrin and does not result in production of thrombin, feedback or amplification of the coagulation cascade. Escherichia coli that express the protein Curli are also known to activate coagulation factors, such as factor XII (ref. 17). This process was shown to cause slower initiation of coagulation due to depletion of factor XII (ref. 17). Bacteria are also well known to directly initiate coagulation in some organisms, such as horseshoe crabs, but this mechanism of controlling infection is believed to have been lost during the evolution of vertebrates18. All of these results prompt the following simple question: are bacteria capable of directly initiating the coagulation cascade and causing coagulation of human blood?” [2008]
This went on to give some results from experiments
- “Clusters of B. cereus initiated coagulation of flowing human whole blood in 3-13 min (Fig. 2b,c), whereas coagulation did not occur until 48-59 min in experiments with the control strain of E. coli (Fig. 2d; P < 0.001)…. both coagulation factor X and prothrombin are required for initiation of coagulation by B. cereus, which is not expected for S. aureus-type coagulase activity.”
- “In addition to B. cereus, we found that clusters of several other Bacillus species, including B. anthracis, the anthrax-causing pathogen, rapidly initiated coagulation of human blood plasma (Fig. 4a). The closely related species Bacillus thuringiensis and other species, including Bacillus subtilis and Bacillus licheniformis, also initiated coagulation. “
- “We predict that other bacterial species that activate coagulation factors may demonstrate this quorum-acting mechanism, although this prediction remains to be tested. Porphyromonas gingivalis, a causative agent of gum disease, is one likely candidate. Purified proteases of P. gingivalis are particularly potent and known to activate many coagulation factors and reduce coagulation times in standard assays11. P. gingivalis infections have also been linked to cardiovascular disease, although the nature of this connection is still under investigation49.”
IN OTHER WORDS _- TAKING ANY BACILLUS PROBIOTICS MAY ENCOURAGE THICK BLOOD.
Bottom Line
We only have partial knowledge on which bacteria can cause coagulation / thick blood. We do see that one of them, Staphylococcus aureus, is strongly associated with CFS (see my last post on the new study from Australia-New Zealand). Of special concern is that a common type of probiotic was demonstrated to cause coagulation!
The reader asked if there was “Is there a viscosity test you recommend for seeing that the thickness is at any given time?”, See Erythrocyte Sedimentation Rate – SED
For more reading on this see these posts (from almost 2 decades ago!)
 Bottom Line
Bottom Line