The patient is in the mid 20’s male and under treatment with a very well known CFS specialist. “although he is stable we aren’t seeing any further improvement…. He doesn’t meet the official CFS definition since he only has the PEM (Post-exertional malaise), general on-going fatigue, and maybe some sleep issues.”
This is the first of two parts, the second part is after the first Pfizer covid shot. This will be interesting to see the shifts.
“Also, after this sample was sent into Thryve he had his first Pfizer covid shot and then had a crash – so I got another sample at that time that I should get results for in a few weeks.”
KEGG Results
KEGG Probiotics
I am going to do a multiway compare in the hope of clustering a consensus from different algorithms. Using advance suggestions
I tend to favor KEGG because the data it is working from is significantly complete. Using Net Benefit and Advance suggestions — we got only weak results (usually against) or no results, except for Lactobacillus paracasei. This would be my first choice for trying a probiotic except it is a histamine producer.
| Probiotic (available commercially) |
| Bacillus thuringiensis or Bacillus mesentericus |
| Clostridium butyricum |
| Bifidobacterium adolescentis |
| Enterococcus faecalis |
| Lactobacillus kefiri |
Probiotic Suggestions Analysis
Look at the Lactobacillus Genus, we see that this person is at the 87%ile (i.e. much higher than most people). Bifidobacterium is 29%ile, i.e. in the normal range. It is not surprising that these two are low as suggestions. On the other side, there was ZERO bacillus reported (not unusual, Thryve only reports Bacillus 45% of the time) which seems to be reflected in the top suggestions being Bacillus probiotics.
Having high lactobacillus can contribute to ME/CFS Symptoms. In general, lactobacillus probiotic should be avoided unless verified to not be d-lactic acid producers (if no information, assume they produce!!)
- Reminder of D-Lactic acidosis and ME/CFS [2019]
- D-lactic Acidosis -Sauerkraut is not good for you if you have CFS! [2015]
- Reducing Lactic Acid Producing Bacteria – LABO [2017] – contains suggestions
KEGG Supplements
As with probiotics, I tend to favor KEGG suggestions for similar reasons. The list below is where their generated values falls in the bottom 5%. All of them are available on Amazon, iHerb and other suppliers
- #1 beta-alanine (quick intro: it may reduce both histamine [2019] and lactic acid[2020] – both of which have cognitive impact.)
- beta-Alanine and gamma-aminobutyric acid in chronic fatigue syndrome [2007]
- Preliminary determination of the association between symptom expression and urinary metabolites in subjects with chronic fatigue syndrome [1996] “strong associations of CFSUM1 and beta-alanine with CFS symptom expression”
- Preliminary determination of a molecular basis of chronic fatigue syndrome [1996] “beta-alanine were positively correlated with symptom incidence, symptom severity, core CFS symptoms”
- iron
- Iron insufficiency and hypovitaminosis D in adolescents with chronic fatigue and orthostatic intolerance [2011]
- Serum concentrations of some metals and steroids in patients with chronic fatigue syndrome with reference to neurological and cognitive abnormalities [2001] ” The results indicate that patients had significantly increased serum aluminum and decreased iron compared to controls”
- L-asparagine
- Hematologic and urinary excretion anomalies in patients with chronic fatigue syndrome [2007] “Significant decreases in the urinary excretion of asparagine”
- L-Lysine
- Nothing explicit, implication that it may help from this study [2017]
- L-Proline
- Comparison of differential metabolites in urine of the middle school students with chronic fatigue syndrome before and after exercise [2018] This is a good match for the PEM issue “The disorder of arginine-proline metabolic pathway is detected in CFS middle school students before exercise intervention.”
- Molybdenum – nothing found
- NADH
- Common supplement suggested for ME/CFS, see this collection on PubMed.
- Phytase (Enzyme) – nothing found
As always consult with your medical professional. A pattern to discuss: start at 1/8 of the suggested dosage and increase every 4 days (usually doubling). Do one at a time, keeping those that have apparent benefit. If you stop giving one, wait 4 days before starting the next, on occasion, stopping may reveal that it helped — just slowly.
Most of the suggestions above appears to agree with studies as illustrated above. We have 3 suggestions that are novel (unstudied) for ME/CFS: Phytase, Molybdenum, L-Lysine.
This strong agreement to studies is reassuring for using the KEGG model. The model knows only the bacteria, no lab tests or diagnosis. Far more critical (for modelling), it appears to explain that the lab results can be reliability attributed to the ME/CFS microbiome population!
Core Supplements
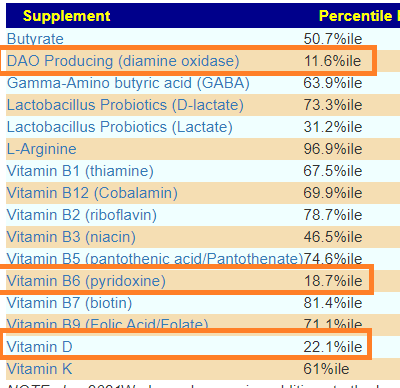
While core supplements has largely been replaced by KEGG, it is still available. There was only one supplement computed that strongly suggests supplementation, DAO. There is no studies on PubMed for CFS and DAO, however DAO does reduce histamine levels — it is a possible experiment to try. I know several people with ME/CFS that have histamine issues, in some cases, severe hay fever. There is some literature in this direction:
- Chronic fatigue syndrome: influence of histamine, hormones and electrolytes [1993]
- “Because of anecdotal reports and uncontrolled trials showing antihistamine efficacy in CFS,”[1996]
The second lowest is Vitamin B6
- Vitamin B status in patients with chronic fatigue syndrome [1999] “data provide preliminary evidence of reduced functional B vitamin status, particularly of pyridoxine, in CFS patients.”
The third lowest is Vitamin D, a well establish lab result for CFS. Generally “low level” supplementation does not work because the ME/CFS microbiome does a poor job absorbing it. A collection of PubMed Studies, and my prior blog posts
- Vitamin 25D and 1,25D measure – one reduces symptoms and one indicates CFS state [2015]
- Vitamin D and the Microbiome [2017]
- Viral Reactivation and the Microbiome [2020]
- Anna Dorothea Hoeck, MD (ME-Pedia.org)
An important observation
All of the above suggestions came solely from the microbiome of the person (no diagnosis information at all!!!). The suggestions agree with significant subsets of ME/CFS patients. Using the microbiome, we appear to be able to be uber-specific to the person. We are not working off “general treatment suggestions” for ME/CFS. The suggestions in this post may not apply to a different ME/CFS patient — they have a different microbiome! Likely similar, but different!
Philosophy
The concept is to supplement what is not being produced by reduced bacteria creating a more normal environment. The hope is that a more normal environment will trigger feedback loops in the microbiome that will increase the reduced (or excessive) bacteria. The microbiome is a city – with a city, reducing the crime rate can often be the result of eliminating causes like: poverty, education, job opportunities, etc.
National Library of Medicine Comparison
In general, the bacteria identified for Chronic Fatigue Syndrome in Studies is not suitable for strong pattern matching. Chronic Fatigue Syndrome has a spectrum with many subsets. This variety is reflected in the studies.
I went to the Component Analysis / Medical Conditions page and then clicked under the Count Column, i.e. by the 📚 for Chronic Fatigue. I then Clicked on Direction to put all of the flagged items (💥) at the top. I then put checked the checkbox besides them (family, genus, species). On this page the 💥 is NOT outside of the Kaltoft-Moltrup Normal Range, but above 75%ile or below 25%ile. The Change Your Microbiome / Medical Condition (PubMed) Outliers applies the 💥 with the K-M ranges (in this sample, there were actually zero outliers!!!)

Why this change? The studies reported averages were above or below for Chronic Fatigue Sydrome compared to controls. The studies did not report extreme values (which is the K-M goal).

Above we have the Hand-Picked Suggestions (which uses only the above).
First, we see that two of my favorites (as a person who has dealt with ME/CFS personally) is at the top of the list: Slippery Elm and Triphala. All of the probiotics suggested are non-lactic acid producers: Bifidobacterium. We do have a disagreement with CORE suggestions on Vitamin B6 (CORE says levels may be low, above says avoid). Given that the avoid list is full of B-Vitamins, I would tend to avoid.
Other ways of Getting Suggestions
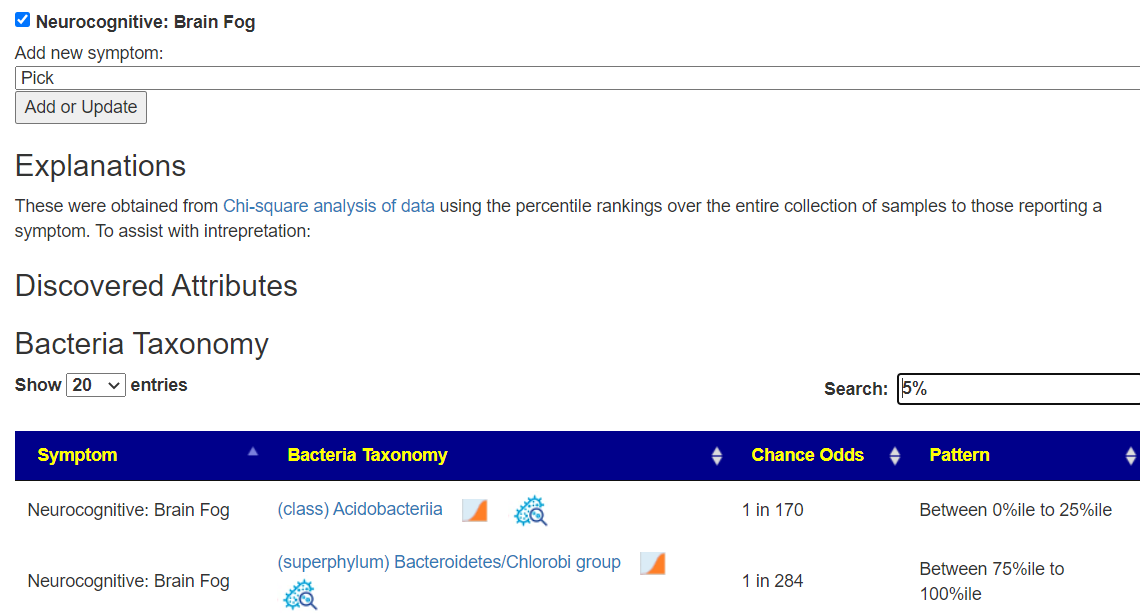
Since ME/CFS often have cognitive challenges, I have a canned computation ( Changing Your Microbiome / For Chronic Fatigue Syndrome./ Brain Fogged ). The suggestions are below.

Above I did the path that I felt was best focused a person for Chronic Fatigue Syndrome. The scopes here is less bacteria and also flags high Lactobacillus. We could add Lactobacillus to the hand picked bacteria (exercise for the reader), but I am inclined not too because lactobacillus will dominate suggestions because there are so many studies for it, the other bacteria will fade off the suggestions.
| Bacteria Name | Analysis |
|---|---|
| Dorea longicatena | Too Low |
| Lactobacillus | Too High |
| Odoribacter splanchnicus | Too Low |
There are some others options on the site:
Dr. Jason Hawrelak Guidance
His results are based on general health and not ME/CFS. With this sample, we see these bacteria being selected. There is nothing in common with our first analysis, and only lactobacillus with our one above.
| Bacteria Name | Analysis |
|---|---|
| Akkermansia | Too Low |
| Bifidobacterium | Too Low |
| Blautia | Too Low |
| Faecalibacterium prausnitzii | Too High |
| Lactobacillus | Too High |
| Roseburia | Too Low |

I would not run with these suggestions — they are simply not focused on ME/CFS.
Symptom Prediction – Citizen Science
The bacteria pattern found with some 1700 prior samples appears to match. This implies that many symptoms are microbiome bacteria caused — something that may be modified. Many of the prediction agrees with what we know. One item is new, Carbohydrate intolerance which is hinted at by our Phytase (Enzyme) recommendation from KEGG.
It also lines up with the iron recommendation and suggests the mechanism for iron being low:
- Potential of Phytase-Mediated Iron Release from Cereal-Based Foods: A Quantitative View [2013]
- ” In the absence of phytase, phytic acid can impede the absorption of other minerals like iron, zinc, magnesium and calcium by binding to them” [2021]

Antibiotics?
The physician being worked with is not dogmatically opposed to using antibiotics. So I did antibiotics only suggestions with the results shown below. Remember this is off label use of these antibiotics.

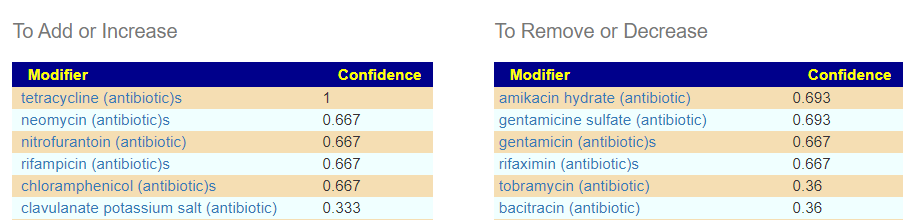
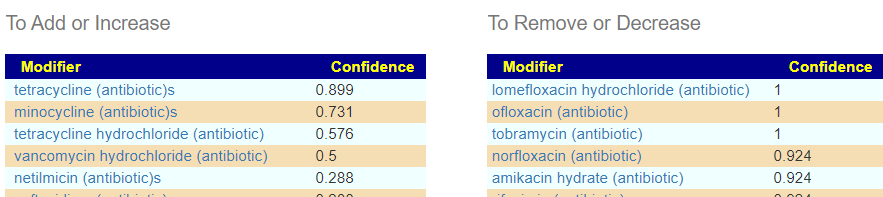
We have everyone agreeing!!! The Tetracycline family (which includes minocycline and doxycycline). My personal preference in minocycline. Not only do we have agreement between methods — we have agreement with protocols reporting success (to various extents) with ME/CFS. [Success or failure is likely connected to each patience’s microbiome]. This approach fell out of favor during the crackdown on “inappropriate use of antibiotics to prevent antibiotic resistance”, and appears to be considered again in 2021.
- Oral Minocycline Therapy Improves Symptoms of Myalgic Encephalomyelitis, Especially in the Initial Disease Stage [2021]
- Could Minocycline be a “Magic Bullet” for the Treatment of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome? [2021]
- Treatment of chronic fatigue syndrome with antibiotics: pilot study assessing the involvement of Coxiella burnetii infection [2005] “we administered tetracycline antibiotics to subjects with CFS … In the QFS group …mean temperatures and headache scores were significantly decreased after treatment (p<0.001). performance status scores were also improved.”
- Nicolson GL, Nasralla M, Franco AR, A. Robert F, Nancy LN, et al. (2000) Diagnosis and integrative treatment of intracellular bacterial infections in chronic fatigue and fibromyalgia syndrome, Gulf War illness, rheumatoid arthritis and other chronic illnesses. Clin Pract Alt Med 1: 92-102.
- Role of Rickettsiae and Chlamydiae in the Psychopathology of Chronic Fatigue Syndrome (CFS) Patients: A Diagnostic and Therapeutic Report [2000]
In this case, “prescribing antibiotics to address a microbiome dysfunction” (which is exactly what we are doing), would likely fly with most medical review boards 🙂
Bottom Line
We have come up with some very specific suggestions based on the person’s microbiome and ME/CFS as a condition. We have also looked at some less specific approaches. These approaches would often be the “stock-in-trade path” that many medical professional will walk. IMHO, they are “ok” but not as “good” or “awesome” as a really focused approach.
Remember, all suggestions should be discussed with a medical professional before doing. The Microbiome Prescription site goal is to model a variety of diseases and compute theoretical candidates for treatment. In some cases, like this post, we find that many candidates have been tested with positive results. Other candidates have not been and thus are potential ones (with logic and studies inferring their benefit).