
I have update my 2018 post, on my MicrobiomePrescription site and I have also done a video on it.
- What is the best diet in your opinion?” [2018]
- What is the best diet in your opinion? – Microbiome Prescription Blog [2022]
I have update my 2018 post, on my MicrobiomePrescription site and I have also done a video on it.
While working on a different blog post on brain fog, the light went on for a model that may explain newly developed alcohol intolerance in ME/CFS. People tolerated and enjoyed alcohol before ME/CFS so the cause is not DNA for these people, but some change caused by ME/CFS.
A major subset of people with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) has excessive lactic acid, typically d-lactic acid, especially with cognitive issues (see Systematic review and meta-analysis of cognitive impairment in myalgic encephalomyelitis / chronic fatigue syndrome (ME/CFS). [2022])
What would consuming alcohol (known as ethanol) do to such a person? The answer is clear from the literature:
So the model is simple:
So the key issue is to reduce lactic acid levels. I have written about this many times over the years, a few examples:
As a FYI, a few people using their microbiome results and my analysis site, Microbiome Prescription, has reported the ability to enjoy a glass of wine when they were intolerant before. There is hope.
The following is suggested reading, https://shop.healthmasters.com.au/pages/chronic-fatigue-syndrome-cfs-treatment-recommendations
It gives an extensive list of suggestions with dosages and the studies they are based on, for example
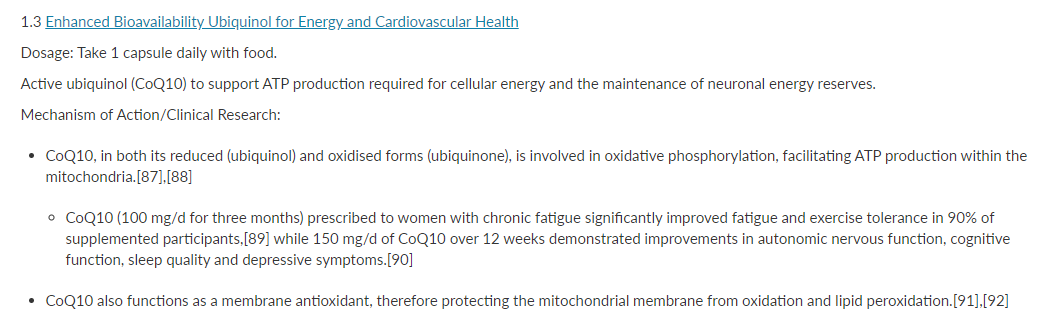
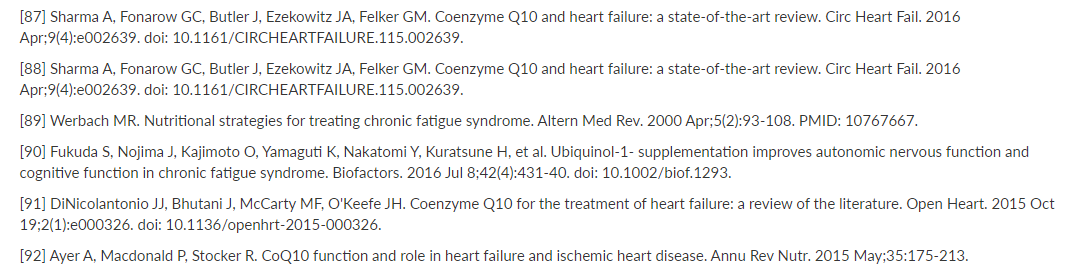
It is a “all on-one-page” that is ideal to discuss with your medical professional.
There are many nuisances in the studies cited that are missed or have misleading inferences. Simple example, “individuals who regularly exercised…. experience less fatigue”… could be restated as “individuals who experience less fatigue…. regularly exercised”. Causality is not in the evidence.
Also, Cognitive-behavioral therapy trials has many more than the single study cited — the majority of studies found that it did not help, or made people worse.
For the last few months I have been working with someone that runs a Long COVID support group. This has resulted in more modifiers being added. One of the outcomes has just been added to the site. She requested that a simplified set of suggestions be added to the site to make her life easier. This consists of items she picked from her experience dealing with the group.
Where to transcribe or upload data (depending on which test)
16s High Resolution tests
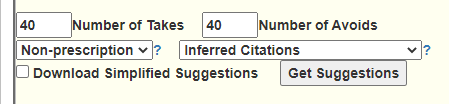
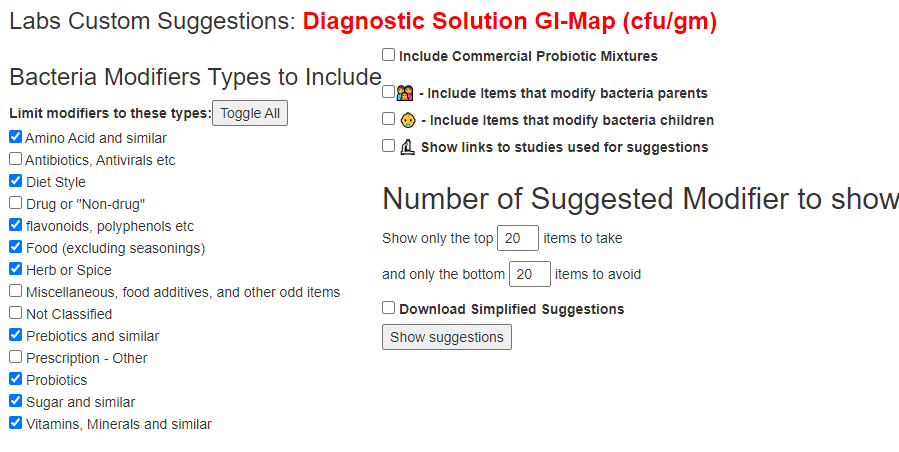
These simplified suggestions has been added everywhere (tell me if I missed a page). If you use GI Map or similar reports, it is available after you have transferred and return to adjust suggestions. You should see these options on most suggestion pages now. To get this new condensed report, just click the checkbox.
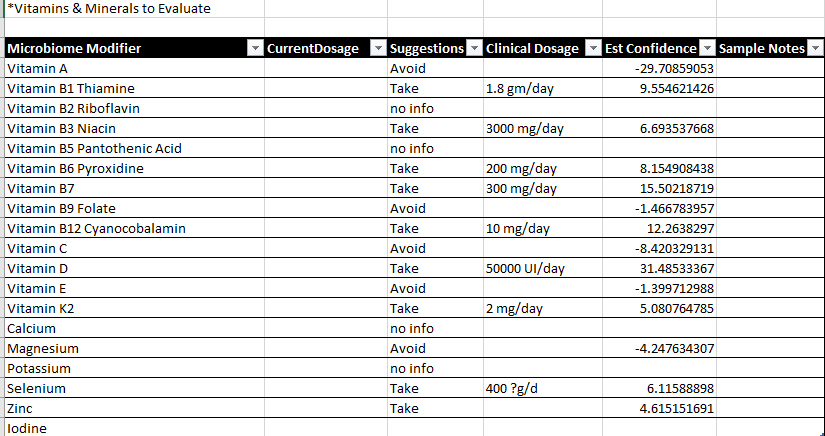
The report is a CDV file (loads into Excel or other spreadsheet programs)

After loading, into Excel, you will need to adjust column widths
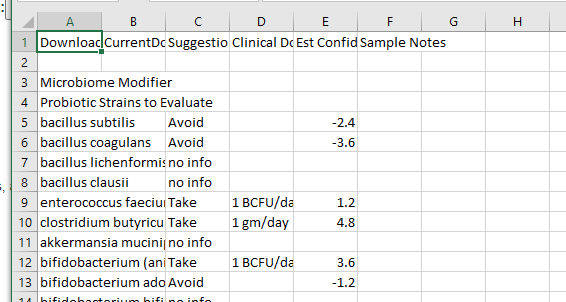
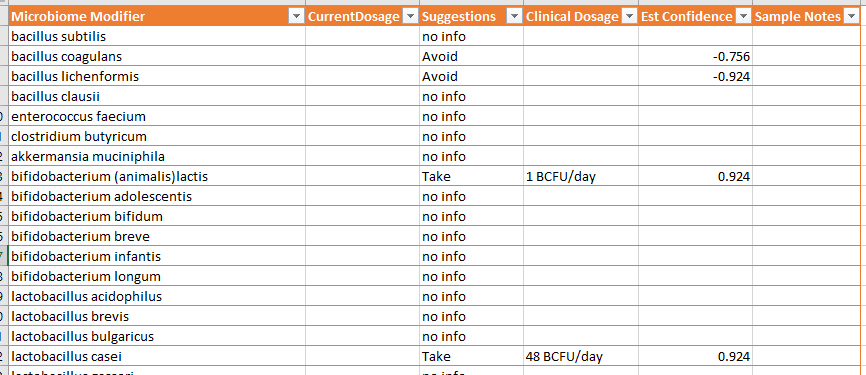
If an item is a Take, then a clinical dosage is given (if known). Clinical Dosages are those reported from studies listed on the U.S. National Library of Medicine Clinical Trials site.
Other sections are shown below.
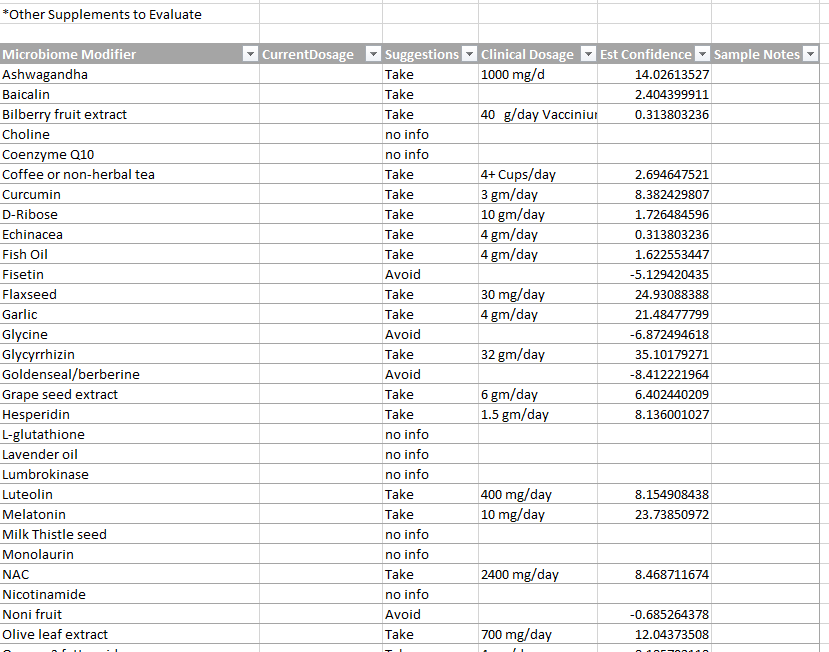
At the bottom of the page are some essential reminders.
Some of the clinical dosages above may be problematic with some medical conditions.
Dosages should be reviewed by a medical professional before starting.
The suggestions are based on a mathematical model. dosages are from clinical studies.
This is a follow up for a reader from 2017 (yes FIVE YEARS ago). It was when I was attempting to work suggestions by hand, before I handed that process to Dr. Artificial Intelligence.
I have not taken any probiotics for over 1 year. My medical treatment is pharmacological for type 2 diabetes, levothyroxine, hydroaltesone[Hydrocortisone], hydroferol[vitamin D3 analog] 1 a month, statins, Omega 3 and fenofibrate, I have not taken probiotics.
Symptoms persist, abdominal bloating, tiredness, unrefreshing sleep, PEM, sore throat, lack of energy, exercise intolerance, visión changes, all symptoms of ME/CFS
Also the increase un body weight has been considerable and it is not possible for me to lose weight, my complexion was thin.
The latest sample was from BiomeSight so the number comparison below is more out of interest than being a truly valid comparison (which would be same lab to same lab). On the surface of the comparison we see what appears to be significant improvement on high percentile bacteria but an increase of low percentile bacteria.
Using the various canned criteria (Jason H, Medivere, Metagenomics, MyBioma, and XenoGene), there has been no change. By “canned”, we mean the bacteria picked by various sources that are important –usually at the genus or family level. The criteria below these lines are sensitive to the lab and the quality of the sample.
| Criteria | Current Sample | Old Sample |
|---|---|---|
| Lab Read Quality | 6.9 | 8.4 |
| Bacteria Reported By Lab | 543 | 203 |
| Bacteria Over 99%ile | 1 | 22 |
| Bacteria Over 95%ile | 10 | 40 |
| Bacteria Over 90%ile | 26 | 51 |
| Bacteria Under 10%ile | 262 | 31 |
| Bacteria Under 5%ile | 205 | 18 |
| Bacteria Under 1%ile | 147 | 2 |
| Different Labs – Items Skipped | ||
| Pathogens | 38 | 18 |
| Outside Range from JasonH | 8 | 8 |
| Outside Range from Medivere | 13 | 13 |
| Outside Range from Metagenomics | 10 | 10 |
| Outside Range from MyBioma | 9 | 9 |
| Outside Range from Nirvana/CosmosId | 13 | 13 |
| Outside Range from XenoGene | 5 | 5 |
| Outside Lab Range (+/- 1.96SD) | 9 | 20 |
| Outside Box-Plot-Whiskers | 61 | 47 |
| Outside Kaltoft-Moldrup | 236 | 89 |
In the old analysis I was using ratios to mean. I have since moved on to percentiles. The table below looks at the top items and compare to percentiles. Note: there can be differences between labs on what they called bacteria (see The taxonomy nightmare before Christmas… (2019)).
| Bacteria (Ratio to mean) | Old Sample Ubiome | New Sample Biomesight |
| Parasutterella: (14.2x) | 99.8%ile | Not Reported |
| Sutterella | 99.7%ile | 95%ile |
| Adlercreutzia: (6.84x) | 99%ile | 0%ile |
| Bilophila: (6.36x) | 99%ile | 88%ile |
| Butyricimonas: (5.28x) | 99%ile | 40%ile |
| Oscillibacter: (3.69x) | 94%ile | Not Reported |
| Intestinimonas: (3.36x) | 97%ile | Not Reported |
| Odoribacter: (3.20x) | 97%ile | 40%ile |
| Flavonifractor: (3.1x) | 99%ile | Not Reported |
| Parabacteroides distasonis | 88%ile | 97%ile |
| Bacteroides ovatus | 36%ile | 98%ile |
| Phocaeicola massiliensis | 95%ile | 99% |
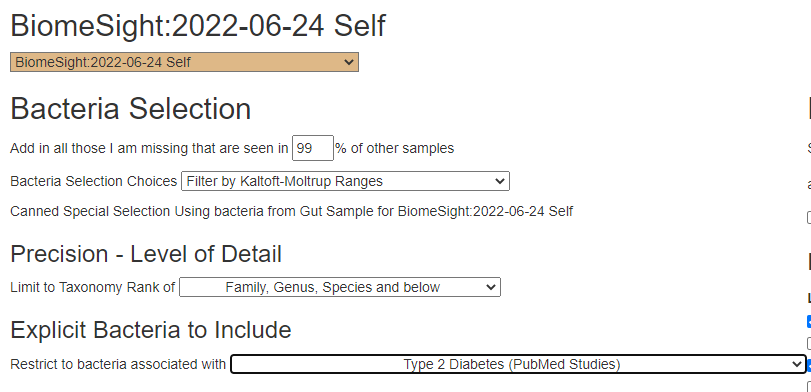
We are doing suggestions from the following:
The goal of doing consensus are two fold:
As a FYI, the PubMed are done via the Research Features / Advance Suggestions. Some produced no suggestions (for example Diabetes — which may be due to the diabetes drugs normalizing the bacteria)
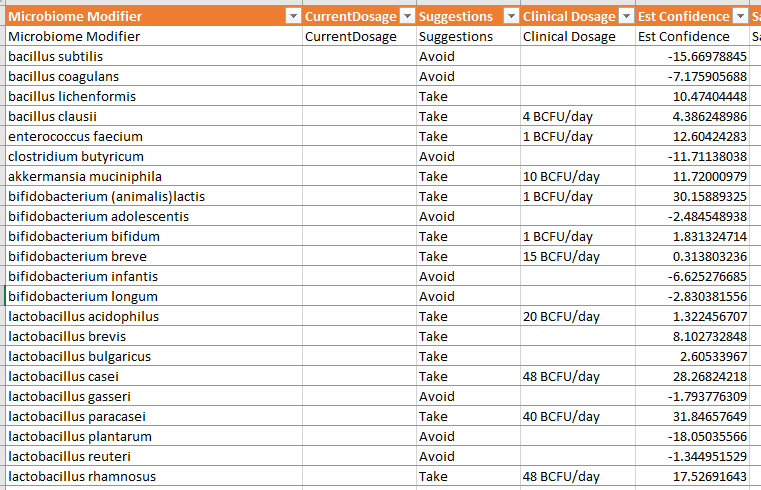
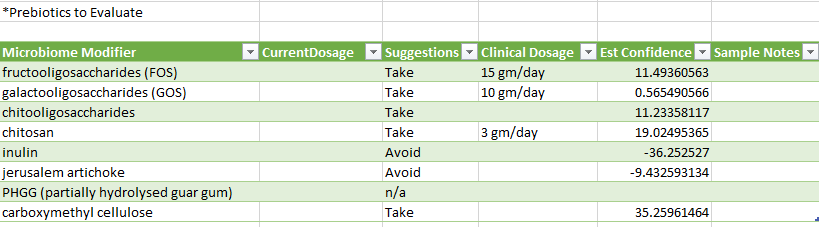
The top items (in descending order) are below. Unusually, every single one was a take recommendation for each set of suggestions generated above. There is a rather clear theme on fibers.
The top suggestions are below in decreasing order.
I noticed that both lactobacillus plantarum (probiotics) and bifidobacterium longum (probiotics) are in the list, as it was for the ME/CFS person in this post: An email from a ME/CFS reader on Probiotics. As with that person, symbioflor 2 e.coli probiotics (US Source, World Wide Source) is lower down on the list. I checked the KEGG AI Suggested Probiotics [revised], and got a low 4.9 for Escherichia coli (with the highest value being just a 7 – indicating reasonably good balance). Using uBiome data, Escherichia coli was the top choice with a big 108.1. I would be inclined to offer the same advance as I did with the email, “because this probiotic is known to persists, use one bottle as part of probiotic rotation” – even just taking once a week is fine.
REMEMBER: The order does not reflect effectiveness — it reflects the amount of research available, hence the term Confidence.
We have a variety of items listed that are usually suggested for ME/CFS. The reason that they are suggested is that blood tests show low levels. I am becoming inclined to suspect that the low levels in the blood is because of greedy bad bacteria in the microbiome that consumes them before it get to the blood. SPECULATION: Taking them as a supplement, feeds the bad bacteria and keeps ME/CFS going.
Vitamin B injections are likely fine, probably good! “ Patients with myalgic encephalomyelitis (ME, also called chronic fatigue syndrome) may respond most favorably to frequent vitamin B12 injections” [2015]
The thing that I have noticed with analysis is that two people have the same diagnosis and common symptoms, but their microbiomes are different and the AI generated suggestions are very different.
With no active work on the microbiome, the microbiome stayed similar. Some of the changes may be due to the drugs being used; fenofibrate,(prescription) – reduces Odoribacter, Bilophila, Flavonifractor and Butyricicoccus (which we saw above)
I would suggest trying the above suggestions (after it is reviewed by your MD), and retest every 4 months. Looking at A History of Several 16s Tests and Suggestions which was done on another ME/CFS person, we saw improvements in the he various canned criteria (Jason H, Medivere, Metagenomics, MyBioma, and XenoGene) after 3-4 months.
