A reader asked me to review a new paper “Chronic bacterial intoxication syndrome under the mask of CFS/ME” that is being discussed a lot on Phoenix Rising. I tend to have an interesting perspective:
- being in remission from CFS/ME I have deep desired to be current but far from desperate
- many people reading and discussing are desperate. Desperation often diminished critical analysis
- I am well trained professionally — not only in the scientific method, but also in statistical analysis.
Key Weakness of CBIS paper
Over the last few decades, it is common for a forlorn hope discovery to be done solely on some finding of a group of ME/CFS patients. The critical test is a simple one: a third party lab confirming the findings with a different group of ME/CFS patients with a matching control/healthy group. The ideal is multiple labs confirming this. Failure to replicate is too frequently the slow death of theories (but many “believers” will continue to advocate the theory – they want something to believe in).
Participants: All patients (children up infancy and adults aged till 80 years) who seeked advice in
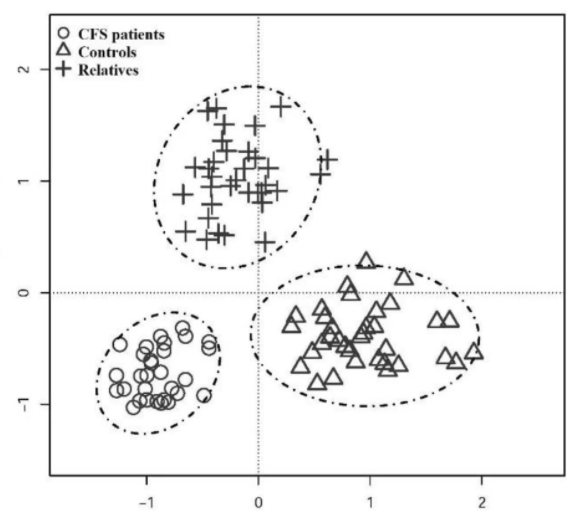
There are no Controls being cited. Additionally all of the patients appears to be from two clinics in the Ukraine. This may be an environmentally homogenous group (shared DNA, shared diet, shared vaccine history).
clinics during 2009-2020 with complaints consistent with a diagnosis of CFS, which was previously
diagnosed in almost a third of patients on former stages of examination and treatment.
In all patients with typical features of CFS there was revealed a focus of chronic bacterial infection
The term “Nephro dysbacteriosis” is not found on PubMed, so how can it be “was called“
in the kidneys, which more often remained clinically locally asymptomatic and was called Nephro
dysbacteriosis.
The issue of being “asymptomatic” is a term of today, with asymptomatic COVID being an echo. The concept is not new, with hypercoagulation model — we have it being asymptomatic in terms of expected symptoms (strokes, Deep Vein Thrombosis etc) but symptomatic with fertility issues. Similarly with Cecile Jadin model, we have “occult infections” which do not appear with typical tests, but are detected with specialized tests.
If it is true, what should be forecasted? Well, a chronic low level kidney infection should manifest itself with kidney diseases and lab tests over time. Over the last many decades, there appears to be only a single paper, with no commonality.
Increases in pain distribution were associated with reductions in serum essential amino acids, urea, serum sodium and increases in serum glucose and the 24-hour urine volume; however the biochemistry was different for each pain area. Regression modelling revealed potential acetylation and methylation defects in the pain subjects.
“Widespread pain and altered renal function in ME/CFS patients[2016]”
Skipping the 14 pages of the paper is reciting history and many more pages on individual histories, we come to identification of the bacteria
Bacteria that had to live naturally in our intestines and work there productively, providing human life. But which, apparently by mistake, but purposefully settled in the kidneys. Most often they were enterococci and enterobacteria-Escherichia coli, Klebsiella, Proteus, Enterobacteriaceae, Morganella, Acinetobacteria, Hafnia,
Seratia and others, in no single cases – Staphylococcus and Streptococcus, less often – Nosocomial Pseudomonas aeruginosa.
“A toxicological blood test, the results of which will be presented in Report 8, was considered as a laboratory confirmation of the diagnosis CBIS.” – problem is this, a blood test is not kidney specific. We could be detecting bacteria escaping from the guts only.
Note also, this is not a test normally available — it is “a toxicological blood test using the “Toxicon” diagnostic system developed by a group of Ukrainian scientists“
What is their treatment?
The treatment are “bacterial vaccines”. This is a concept not well known in the west and will likely be at least a decade before any significant approval would be granted in the west. A 2018 review is well worth readin , Vaccine development for enteric bacterial pathogens: Where do we stand? (Full article PDF). Two quotes from the paper:
“During the first course of immunization with bacterial autovaccine, the intensity of pain in all patients decreased
significantly, and after 2-3 courses – completely passed. During follow-up observation there were no recurrences of trigeminitis.”
“There was prepared bacterial auto vaccine and was carried out immunization with a course of 10 injections. Already during vaccination and for the next 2 years of the follow-up observation there were no more abdominal pain attacks.”
Attitude Issues
The following indicate bravado and bias — they can be effective in winning an audience and a following. Often this helps with raising funds for the person to continue research.
- the new revolutionary previously unknown diagnosis Chronic Bacterial Intoxication Syndrome (CBIS) that gives such a long-awaited in-depth clinical understanding and discovery of the true basic etiological and pathogenetic causes of the long-known and worldwide-spread, but still etiologically mysterious CFS/ME”
- “Moreover, it was found that in at least 90% of patient’s nephron dysbacteriosis and CBIS had developed precisely after thoughtless, expansive and aggressive antibiotic therapy, which often began in childhood.” — someone is on soap box describing a popular demon.
Bottom Line
A vaccine against a kidney bacteria will also have direct impact on the same bacteria in the gut microbiome. On the flip side, appropriate antibiotics would also impact the same bacteria in the Jadin’s protocol using antibiotics will also impact kidney infections.
There is one important difference: vaccines have a longer life of action(typically a year or more) than an antibiotics. Also be aware that the study cited that up to 10 courses of vaccines were needed with some. This sounds a bit like 10 rounds of antibiotics!!
Is it Kidney or Gut? Do we need to use a vaccine or bacteria phages or antibiotics or other forms of microbial manipulations?
Their asserted results are similar to that asserted from both Jadin’s antibiotics protocol and the Hemex protocol (which often uses antibiotics with anticoagulants like heparin).
In 30/35 (85.7%) cases there was almost complete clinical remission in the course of both fibromyalgia and in general CBIS, which in 23/35 (65.7%) patients lasted from 3 to 5 years (observation period).
page 48
The statement that in the basis of chronic fatigue in various diseases there is a single pathogenetic mechanism – persistent chronic bacterial intoxication due to nephrodisbacteriosis may be a little premature.
page 82.
To my mind, for treatment of CFS/ME, the root cause is excessive growth of multiple bacteria with both this model and my microbiome model. The goal is to correct this — vaccine, antibiotics, phages, diet and supplement changes? Whatever works. The key factor is that it is NOT a cure, it is a remission — one that needs to be worked on to maintain.
Until vaccines become available, appropriate multiple courses of the right antibiotics is available today (MD willing!!!). Unfortunately, most MDs are not trained on addressing multiple bacterial infection without nuking the gut.