To me, this keeps getting reported in the literature over the last 30 years, with the latest excitement being this August 2021,
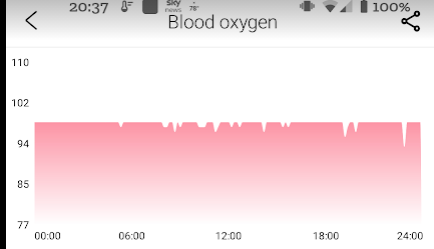
Hypoperfusion or reduced perfusion means simply reduced oxygen gets to the brain. There can be many causes, for example (with convention causes first, then likely ME/CFS/LC causes:
- Low blood pressure
- Heart Issues
- Loss of blood volume
- Hypercoagulation (thick blood)
- Sticky blood
- Inflammation of blood vessels (due to chronic low grade infections — often secondary infections and not primary infections)
- Issues with hemoglobin (iron) due to things like chemical pollutants, including carbon monoxide
Each one of these impair oxygen to the brain and thus can cause many symptoms: inability to concentrate, memory issues, mood swings / irritability, light intolerance, noise intolerance, and many many more. Hypoperfusion also occurs with many neurological conditions and forms of dementia.
To add a personal note, during one relapse of ME/CFS my SPECT scan showed significant hypoperfusion which the radiologist read as “possible early onset Alzheimer’s disease”(due to my age) – it was not, I fully recovered (as evidence by some 1500 blog posts on this site and it’s sister site, Microbiome Prescription Blog.
ME/CFS Literature
When patients deal with MDs, having a rich collection of studies often persuade them to take something serious instead of dismissing it as something from the internet rumor-mill. So, I have assembled prior studies below. Note that POTS has been a hallmark of ME/CFS and is associated with hypoperfusion.
- Assessment of regional cerebral perfusion by 99Tcm-HMPAO SPECT in chronic fatigue syndrome.Ichise M, Salit IE, Abbey SE, Chung DG, Gray B, Kirsh JC, Freedman M.Nucl Med Commun. 1992 Oct;13(10):767-72.
- Brainstem perfusion is impaired in chronic fatigue syndrome.Costa DC, Tannock C, Brostoff J.QJM. 1995 Nov;88(11):767-73.
- Comparison of 99m Tc HMPAO SPECT scan between chronic fatigue syndrome, major depression and healthy controls: an exploratory study of clinical correlates of regional cerebral blood flow.Fischler B, D’Haenen H, Cluydts R, Michiels V, Demets K, Bossuyt A, Kaufman L, De Meirleir K.Neuropsychobiology. 1996;34(4):175-83. doi: 10.1159/000119307.
- Brainstem perfusion in CFS.Nixon PG.QJM. 1996 Mar;89(3):237. doi: 10.1093/qjmed/89.3.237.
- Brain positron emission tomography (PET) in chronic fatigue syndrome: preliminary data.Tirelli U, Chierichetti F, Tavio M, Simonelli C, Bianchin G, Zanco P, Ferlin G.Am J Med. 1998 Sep 28;105(3A):54S-58S. doi: 10.1016/s0002-9343(98)00179-x
- Comparison of SPET brain perfusion and 18F-FDG brain metabolism in patients with chronic fatigue syndrome.Abu-Judeh HH, Levine S, Kumar M, el-Zeftawy H, Naddaf S, Lou JQ, Abdel-Dayem HM.Nucl Med Commun. 1998 Nov;19(11):1065-71. doi: 10.1097/00006231-199811000-00006.
- Impaired oxygen delivery to muscle in chronic fatigue syndrome.McCully KK, Natelson BH.Clin Sci (Lond). 1999 Nov;97(5):603-8; discussion 611-3.
- Cerebral perfusion in chronic fatigue syndrome and depression.MacHale SM, Lawŕie SM, Cavanagh JT, Glabus MF, Murray CL, Goodwin GM, Ebmeier KP.Br J Psychiatry. 2000 Jun;176:550-6. doi: 10.1192/bjp.176.6.550.
- Single-photon emission computerized tomography and neurocognitive function in patients with chronic fatigue syndrome.Schmaling KB, Lewis DH, Fiedelak JI, Mahurin R, Buchwald DS.Psychosom Med. 2003 Jan-Feb;65(1):129-36. doi: 10.1097/01.psy.0000038942.33335.9b.
- Decreased upright cerebral blood flow and cerebral autoregulation in normocapnic postural tachycardia syndrome.Ocon AJ, Medow MS, Taneja I, Clarke D, Stewart JM.Am J Physiol Heart Circ Physiol. 2009 Aug;297(2):H664-73. doi: 10.1152/ajpheart.00138.2009. Epub 2009 Jun 5. — this is POTS, common with ME/CFS
- Postural neurocognitive and neuronal activated cerebral blood flow deficits in young chronic fatigue syndrome patients with postural tachycardia syndrome.Stewart JM, Medow MS, Messer ZR, Baugham IL, Terilli C, Ocon AJ.Am J Physiol Heart Circ Physiol. 2012 Mar 1;302(5):H1185-94. doi: 10.1152/ajpheart.00994.2011. Epub 2011 Dec 16.
- Right arcuate fasciculus abnormality in chronic fatigue syndrome.Zeineh MM, Kang J, Atlas SW, Raman MM, Reiss AL, Norris JL, Valencia I, Montoya JG.Radiology. 2015 Feb;274(2):517-26. doi: 10.1148/radiol.14141079. Epub 2014 Oct 29.
- A Comparison of Neuroimaging Abnormalities in Multiple Sclerosis, Major Depression and Chronic Fatigue Syndrome (Myalgic Encephalomyelitis): is There a Common Cause?Morris G, Berk M, Puri BK.Mol Neurobiol. 2018 Apr;55(4):3592-3609. doi: 10.1007/s12035-017-0598-z. Epub 2017 May 17.
- The etiologic relation between disequilibrium and orthostatic intolerance in patients with myalgic encephalomyelitis (chronic fatigue syndrome).Miwa K, Inoue Y.J Cardiol. 2018 Sep;72(3):261-264. doi: 10.1016/j.jjcc.2018.02.010. Epub 2018 Mar 24.
- Task Related Cerebral Blood Flow Changes of Patients with Chronic Fatigue Syndrome: An Arterial Spin Labeling Study.Staud R, Boissoneault J, Craggs JG, Lai S, Robinson ME.Fatigue. 2018;6(2):63-79. doi: 10.1080/21641846.2018.1453919. Epub 2018 Mar 20.
- Red blood cell deformability is diminished in patients with Chronic Fatigue Syndrome.Saha AK, Schmidt BR, Wilhelmy J, Nguyen V, Abugherir A, Do JK, Nemat-Gorgani M, Davis RW, Ramasubramanian AK.Clin Hemorheol Microcirc. 2019;71(1):113-116. doi: 10.3233/CH-180469.
- Evidence of widespread metabolite abnormalities in Myalgic encephalomyelitis/chronic fatigue syndrome: assessment with whole-brain magnetic resonance spectroscopy.Mueller C, Lin JC, Sheriff S, Maudsley AA, Younger JW.Brain Imaging Behav. 2020 Apr;14(2):562-572. doi: 10.1007/s11682-018-0029-4.
- Paradigm shift to disequilibrium in the genesis of orthostatic intolerance in patients with myalgic encephalomyelitis and chronic fatigue syndrome.Miwa K, Inoue Y.Int J Cardiol Hypertens. 2020 May 20;5:100032. doi: 10.1016/j.ijchy.2020.100032. eCollection 2020 Jun.
In 20+ years reading literature on ME/CFS, the following issues (or a combination) appear to be dominant causes:
- Hypercoagulation — David Berg, Hemex labs was the original reported in 1998 (Summary) – I had many in person and phone conversations with him before he retired.
- This includes not just thick circulating blood, but also fibrin fragments and deposits that slows the flow of blood
- English translation: Not only the wrong weight of motor oil in the body, but the oil filters are clogged!
- Low Blood Volume — David Bell (summary) in 1995, who I have also had phone conversations with
- Blood Cell Disfigurement — Les Simpson in 1997,
- Smaller heart size (which amplifies other causes) – Kunihisa Miwa and Masatoshi Fujita in 2008 2009, 2011
- Evidence of altered cardiac autonomic regulation in myalgic encephalomyelitis/chronic fatigue syndrome: A systematic review and meta-analysis.Nelson MJ, Bahl JS, Buckley JD, Thomson RL, Davison K.Medicine (Baltimore). 2019 Oct;98(43):e17600. doi: 10.1097/MD.0000000000017600.
There are a few subsets, like those that suffered organophosphate pesticides exposure (2003). Prolonged ME/CFS reduces the size of the brain (I suspect due to prolonged oxygen starvation)
- Gray matter volume reduction in the chronic fatigue syndrome.de Lange FP, Kalkman JS, Bleijenberg G, Hagoort P, van der Meer JW, Toni I.Neuroimage. 2005 Jul 1;26(3):777-81. doi: 10.1016/j.neuroimage.2005.02.037. Epub 2005 Apr 7.
- Regional grey and white matter volumetric changes in myalgic encephalomyelitis (chronic fatigue syndrome): a voxel-based morphometry 3 T MRI study.Puri BK, Jakeman PM, Agour M, Gunatilake KD, Fernando KA, Gurusinghe AI, Treasaden IH, Waldman AD, Gishen P.Br J Radiol. 2012 Jul;85(1015):e270-3. doi: 10.1259/bjr/93889091. Epub 2011 Nov 29
- Gray matter volumes in patients with chronic fatigue syndrome.Tang LW, Zheng H, Chen L, Zhou SY, Huang WJ, Li Y, Wu X.Evid Based Complement Alternat Med. 2015;2015:380615. doi: 10.1155/2015/380615. Epub 2015 Feb 22.
- Progressive brain changes in patients with chronic fatigue syndrome: A longitudinal MRI study.Shan ZY, Kwiatek R, Burnet R, Del Fante P, Staines DR, Marshall-Gradisnik SM, Barnden LR.J Magn Reson Imaging. 2016 Nov;44(5):1301-1311. doi: 10.1002/jmri.25283. Epub 2016 Apr 28.
- Grey and white matter differences in Chronic Fatigue Syndrome – A voxel-based morphometry study.Finkelmeyer A, He J, Maclachlan L, Watson S, Gallagher P, Newton JL, Blamire AM.Neuroimage Clin. 2017 Sep 28;17:24-30. doi: 10.1016/j.nicl.2017.09.024. eCollection 2018.
COVID Literature
The above was the result of 30+ years of investigations, Long COVID is less than 2 years.
- Management of acute ischemic stroke in patients with COVID–19 infection: Report of an international panel. 2020 May 3. – higher risk of stroke (i.e. coagulation)
- Neurovascular and perfusion imaging findings in coronavirus disease 2019: Case report and literature review. 2020 Oct;33(5):368-373. doi: 10.1177/1971400920941652. Epub 2020 Jul 15
- Retrospective Observational Study of Brain MRI Findings in Patients with Acute SARS–CoV–2 Infection and Neurologic Manifestations. 2020 Dec;297(3):E313-E323. doi: 10.1148/radiol.2020202422. Epub 2020 Jul 17. “with perfusion abnormalities (47.7%), “
- Association of Clinical, Biological, and Brain Magnetic Resonance Imaging Findings With Electroencephalographic Findings for Patients With COVID–19..JAMA Netw Open. 2021 Mar 1;4(3):e211489. doi: 10.1001/jamanetworkopen.2021.1489. “Of 57 patients who underwent brain MRI, 41 showed abnormalities, including perfusion abnormalities, acute ischemic lesions, multiple microhemorrhages, and white matter-enhancing lesions”
- Endothelial dysfunction in COVID– 19 and cognitive impairment]. 2021;121(6):93-99. doi: 10.17116/jnevro202112106193. “The development of endothelial dysfunction in COVID-19 can disrupt organ perfusion and cause a procoagulant state, leading to both macro- and microvascular thrombotic events. Cognitive impairment is a common complication of COVID-19 that develop in acute and delayed periods and is not directly related to the severity of the underlying disease.”
Putting it all together
First, try to get an Appropriate Brain Scan depending on the method of scan, abnormalities would be be found from 14% to 80% of the time. You want the 80% scan — or else you MD will say “it’s in your head” in the alternative meaning 😦 .
Second, it is very unlikely that you can be tested for each and every candidate item above. In some cases, there may not be the expertise available or the testing deemed experimental/for research purposes only — this can be ignored/dismissed by a treating physician (or their supervisor). For myself, I had coagulation testing with Berg (their test suite is available in a few locations). There are almost a dozen makers examined — most MDs and even specialists — will only test for a few.
I have put together a collection of researched pages dealing with various issues:
- The Heart and Blood of CFS 2016
- Killing Lactobacillus to improve Brain Fog 2018
- Coagulation: Thick Blood Supplements for CFS and Long COVID 2015 (update 2021)
- Health Rising Reposts: Microbiome and Coagulation 2013
- Red Blood Cells and CFS 2014
The secondary infections are harder to deal with — often they can become occult (using Jadin’s term from the Pasteur Institute for Tropical Medicine), that is, they may not be seen in the blood (an oxygen rich environment) but in the tissue (lower oxygen, and even more when they produce metabolites (toxins) to inflame blood vessels (further reducing oxygen) and cause fibrin barriers to block oxygen from red blood cells getting into the tissue. They may also persist in the gut microbiome and never enter the blood system — instead their metabolites enter the blood system.
Personally, I favor the microbiome alteration approach. The goal is to make a hostile environment for these bacteria by starving them of their preferred food and flooding them with what they do not like. I did the Jadin’s antibiotic protocol (multiple rotating specific antibiotics for months) with earlier relapse — but I have been just as successful with microbiome manipulation with later relapses (and an apparent shorter time to recovery).
There is Hope
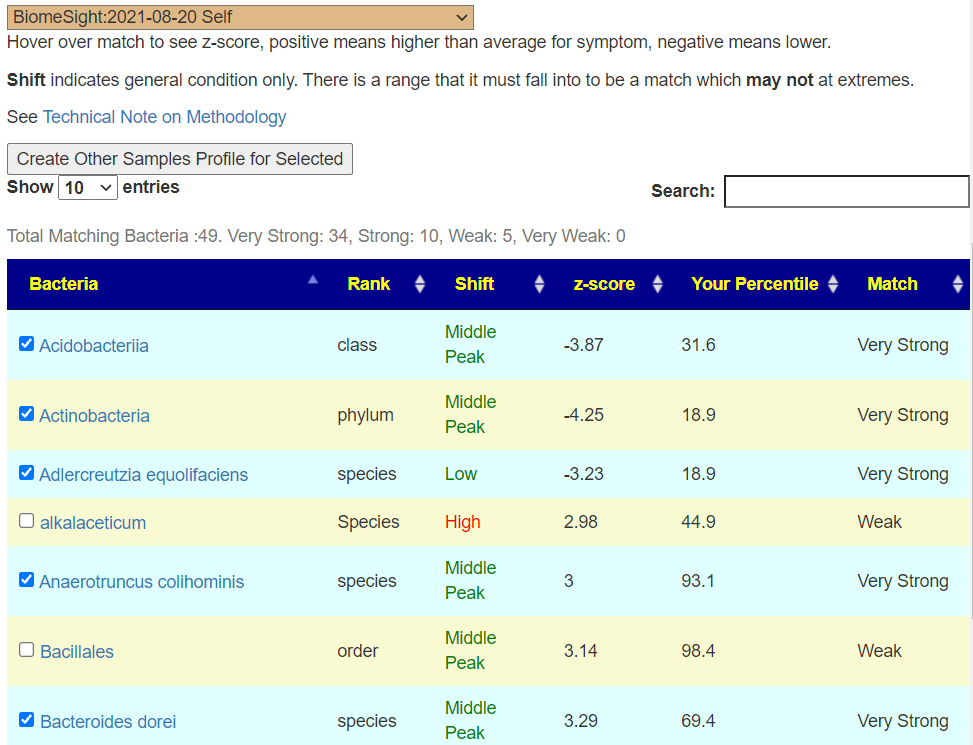
Given the number of issues, challenges with MDs, etc, I realize that most patients will likely get zero traction from the conventional medical establishment — unfortunately. I view that there is a viable alternative treatment approach because of the availability of direct-to-retail 16s microbiome tests. We know that there are pattern of bacteria shifts seen in CFS/ME and Long COVID. It is likely (at least from personal experience) that correcting these shifts result in reduce symptom severity and number (and even complete elimination). See my personal experience here.
The key is really simple — alter diet and supplements –NOT WITH A FORMA COOKBOOK MODEL from Internet ramblings of others — but explicitly based on your personal microbiome. The suggested changes are generated (for free) by artificial intelligence on Microbiome Prescription using almost 2 million facts harvested from the US National Library of Medicine. The suggestions are unique to you — but should always be reviewed by your medical professional before starting.