Hi Ken, tomorrow I have an appointment with a cardiologist, and I want to check for thick blood/coagulation if possible. What blood values would I need to test? Fibrinogen, Prothrombin Fragment 1+2, Thrombin/ AntiThrombin Complexes, Soluble Fibrin Monomer, and Platelet Activation. Is that right?
This has been part of my model of ME/CFS for a long time. It is a co-factor to things like the microbiome. A summary of the old treatment advice from Hemex and transcripts of talks with Dave Berg is here.
Soluble Fibrin Monomer (SFM) – Normal Range 0-15mg/L
Fibrinogen – Normal Range 200-300
Prothrombin Fragment 1+2 test
Antithrombin III (AT),
Protein C,
Protein S,
APC Resistance
Factor II level or the Prothrombin Gene Mutation
Lp(a)
PAI-1
SED (Below 5 is a concern per Berg)
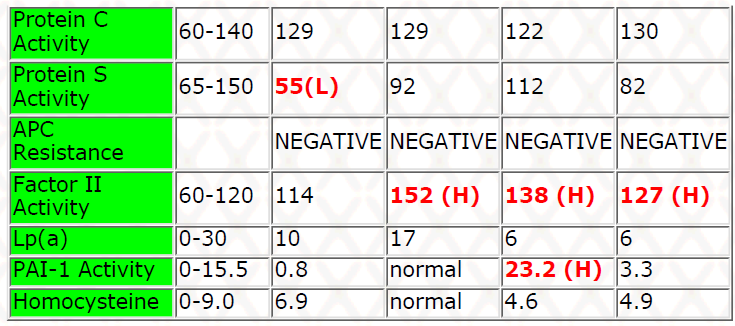
Example of the Family Reports from Hemex
This is from my ancient 2000’s CFS blog that is available here
The patient has done another sample and this continues the analysis. The original post, A German CFS Patient Experience and Analysis from July 2021. I am always interested in seeing changes that occur from the AI suggestions, they worked for me –I am as interested in them not working (to motivate improving algorithms).
What has changed?
There are a set of automatic comparison tools between samples, so I will check those first
I went to compare taxonomy outliers for the two samples and found just two items were on both. There was a lot of changes. We can ignore blues with no data besides – they were all likely what I term transitory bacteria that comes and goes. What we are interested
End Product — most were unchanged except for Polyhydroxyalkanoic acids which jumped from none to 98%ile
KEGG Bacteria Products nothing in common, on first sample we had only low values at risk, on latest sample only high values at risk
KEGG Enzymes — the same thing, earlier sample has all risks being low samples, latest high values
KEGG Modules — earlier sample had no risk items, latest had one high value
Medical Condition (PubMed) — nothing for either sample
The overall impression is that things have changed significantly. This does not say that the person is better — only that the suggestions have changed the microbiome
Non-Automated Comparisons
Next I will look at various aspects and do side by side comparisons. First, using Dr. Jason Hawrelak Criteria, shown below. The worst shift was for Blautia, the best shifts was for Roseburia and Faecalibacterium prausnitzii
Health Status changes were a toss up, but appears marginally better
Latest: 0 Healthy, 4 unhealthy
Earlier: 2 Healthy, 6 unhealthy
KEGG Suggested Probiotics
Earlier Sample had 11 probiotics listed with a maximum weight of 12 (most of the time I see much higher weights indicating greater dysfunction)
Later Sample had 0 probiotics – this is actually a rare occurrence which hints at a better balance microbiome
KEGG Suggested Supplements
Earlier sample has 3 items suggested (using default percentile)
Later sample has 0 items suggested (using default percentile)
Pub Med CFS Profile
Earlier sample had 5 low matches, 5 high matches
Later sample has just 4 high matches
Citizen Science Models
Early Sample: Total Matching Bacteria :26. Very Strong: 15, Strong: 8, Weak: 2, Very Weak: 1
Later Sample: Total Matching Bacteria :24. Very Strong: 19, Strong: 4, Weak: 1, Very Weak: 0
Less matching bacteria (means some have disappeared), while strong/very strong are the same, the weak association have dropped
From looking at all of the available objective measures:
The microbiome has changed (our primary goal)
Many measurements show indicate that the microbiome is moving towards normal, none has a suggestion of things getting worst.
Remember our goal is not to attempt a one-step cure
Our earlier post used this diagram, we appear to have successfully moved along the path to recovery. We need to see what our next step is.
Symptoms Forecasts To Reported Symptoms
This reader was a good user and entered their symptoms – we have a 80% match rate. What is interesting is that one of the items not checked was a Keto Diet — this is interesting because a recent post dealt with a Keto diet resulting in Chronic Fatigue Like symptoms, with “Keto Flu” is some studies. A Keto diet is DEFINITELY NOT A SUGGESTION for this person, it will likely make things worst.
Updated Suggestions
For the earlier post, the consensus reports were not available. My intent is to run each of the matched predicted symptoms, the PubMed profile for ME/CFS and Citizen Science for ME/CFS – a total of 18 sets of suggestions will be merged. There are two ways of doing this:
Only the Auto Checked (which picks a few best items)
Auto Checked plus suggested one (marked with a light bulb).
This first pass is only with auto checked items (the most conservative approach) The bacteria selected are shown below, while there was some duplicates between symptoms, there was significant independence:
Acidobacteria Too Low
Anaerovibrio Too High
Anaerovibrio lipolyticus Too High
Bacteroides cellulosilyticus Too High
Bacteroides finegoldii Too High
Bacteroides salanitronis Too High
Bifidobacteriaceae Too Low
Bifidobacteriales Too Low
Bilophila Too High
Bilophila wadsworthia Too High
Candidatus Phytoplasma Too High
Clostridium malenominatum Too Low
Deinococcaceae Too High
Deinococcales Too High
Deinococcus Too High
Lelliottia Too Low
Lelliottia amnigena Too Low
Mitsuokella Too High
Oscillospira Too High
Parabacteroides johnsonii Too High
Rhodocyclaceae Too Low
Sphingobacterium bambusae Too High
Sutterella stercoricanis Too Low
I noted that many are atypical bacteria that I do not see usually in pub med studies.
Safest Takes is full of items that I often have seen on my own (and other ME/CFS results).
On the Safer Take, we find a regular pattern of 3 takes and 1 oppose.
Whey has historically been helpful to a subset of ME/CFS patients
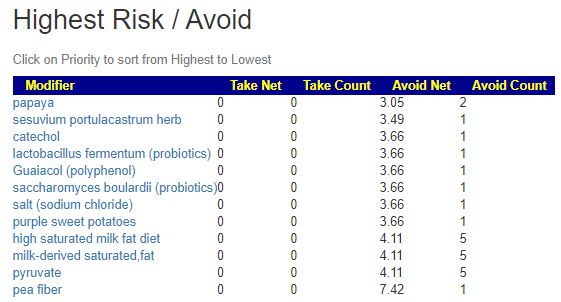
The avoid list is relatively short and most are from a single suggestion (which suggests that it may be ignored). high red meat is the greatest avoid, with saturated fats variation being right behind.
Done with Secondary Suggestions
Since I have just implemented this feature, I am curious about it’s impact. The number of bacteria almost doubled with a variety. A lot of bacteria appeared multiple time.
Absiella Too Low
Acidobacteria Too Low
Acidobacteriaceae Too Low
Acidobacteriales Too Low
Acidobacteriia Too Low
Adlercreutzia Too Low
Adlercreutzia equolifaciens Too Low
Anaerovibrio Too High
Anaerovibrio Too High
Anaerovibrio lipolyticus Too High
Bacteroides cellulosilyticus Too High
Bacteroides finegoldii Too High
Bacteroides salanitronis Too High
Bacteroides vulgatus Too High
Bifidobacteriales Too Low
Bifidobacterium Too Low
Bilophila Too High
Bilophila wadsworthia Too High
Blautia hansenii Too High
Butyricimonas Too High
Candidatus Phytoplasma Too High
Clostridium malenominatum Too Low
Collinsella intestinalis Too Low
Coriobacteriia Too Low
Deinococcaceae Too High
Deinococcales Too High
Deinococcus Too High
Eubacterium dolichum Too Low
Eubacterium oxidoreducens Too Low
Finegoldia magna Too Low
Hymenobacter Too High
Lelliottia Too Low
Lelliottia amnigena Too Low
Leptospira Too Low
Leptospiraceae Too Low
Leptospirales Too Low
Megasphaera Too Low
Mitsuokella Too High
Oscillospira Too High
Parabacteroides johnsonii Too High
Peptococcaceae Too High
Porphyromonas Too High
Pseudanabaenaceae Too High
Pseudonocardiaceae Too Low
Rhodocyclaceae Too Low
Rickettsiaceae Too Low
Rickettsieae Too Low
Selenomonas artemidis Too Low
Slackia Too High
Sphingobacterium bambusae Too High
Streptococcus thermophilus Too High
Sutterella stercoricanis Too Low
Synechococcaceae Too High
Synechococcales Too High
Veillonellaceae Too High
Veillonellales Too High
As expected, the suggests are similar
The risk items are similar with saturated fats dominating
B Vitamins (classic CFS MD recommended supplements)
Vitamin D
Soy
Human milk oligosaccharides (prebiotic, Holigos, Stachyose)
In general, I favor “intact” fiber and herbs. I have seen several studies that the intact had a greater impact than the extract. Watch out for saturated fats — for example Pork is on the to avoid list
The excel file download (CSV) had only 291 items, less than other samples that I processed. I attached it as an example.
My usual advice is to take two weeks to sort out (and in some cases slowly move up to) the suggestions that are picked. It is helpful to check my Supplement Dosage page. That page is not numbers that I picked out of the air, but dosages used in various clinical trials (thus the dosages are likely safe, and more important, are sufficient to cause a change). Then at least 4 weeks for the microbiome to stabilize, then retest to find out the new status quo that will need to be adjusted.
For myself, I did notice a pendulum swing in my series of samples — an item was a take, then the next sample it was an avoid, then it became a take again and stayed as a take. The path is not always straight!
This post was kick-started by a post to a study on a Spanish ME/CFS site shown below
Natto extract, a Japanese fermented soybean food, directly inhibits viral infections including SARS–CoV-2 in vitro.Oba M, Rongduo W, Saito A, Okabayashi T, Yokota T, Yasuoka J, Sato Y, Nishifuji K, Wake H, Nibu Y, Mizutani T.Biochem Biophys Res Commun. 2021 Sep 17;570:21-25. doi: 10.1016/j.bbrc.2021.07.034. Epub 2021 Jul 13. “our study suggests that the putative serine-protease(s) in natto may impair the infectious function of BHV-1 and SARS-CoV-2, probably through the proteolysis of its glycoprotein D and the spike protein, respectively.”
This is extra relevant because Nattokinase is one of my personal favorite tools for dealing with hypo-perfusion (low oxygen to the brain), something that I have experienced during ME/CFS flares. It is also the subject of my last post. I have cited Nattokinase in prior posts, some 9 years ago, and it seems time to update what we know.
So what more has been added to our knowledge base. Nattokinase comes from Bacillus Subtilis Natto. This strain has been traditionally used in a Japanese dessert called “Natto” which you can buy is some Asian shops – it is a bit of an acquired taste (but I like it)
What Natto looks like in stores. This is a living bacteria.
Fibrinolytic characteristics of Bacillus subtilis G8 isolated from natto.Pinontoan R, Elvina, Sanjaya A, Jo J.Biosci Microbiota Food Health. 2021;40(3):144-149. doi: 10.12938/bmfh.2020-071. Epub 2021 Feb 20. “Both nattokinase and B. subtilis G8 were able to dissolve both whole blood and euglobulin clots.” – important for COVID micro-clots.
Data Recorded in Real Life Support the Safety of Nattokinase in Patients with Vascular Diseases.Gallelli G, Di Mizio G, Palleria C, Siniscalchi A, Rubino P, Muraca L, Cione E, Salerno M, De Sarro G, Gallelli L.Nutrients. 2021 Jun 13;13(6):2031. doi: 10.3390/nu13062031. “we can conclude that the use of nattokinase represents an efficient and safe treatment able to both prevent and treat patients with vascular diseases.”
[A clinical study on the effect of nattokinase on carotid artery atherosclerosis and hyperlipidaemia].Ren NN, Chen HJ, Li Y, Mcgowan GW, Lin YG.Zhonghua Yi Xue Za Zhi. 2017 Jul 11;97(26):2038-2042. doi: 10.3760/cma.j.issn.0376-2491.2017.26.005. “daily NK supplementation is an effective way to manage the progression of atherosclerosis and potentially may be a better alternative to statins which are commonly used to reduce atherosclerosis and further to prevent cardiovascular attack and stroke in patients.”
Hypoperfusion or reduced perfusion means simply reduced oxygen gets to the brain. There can be many causes, for example (with convention causes first, then likely ME/CFS/LC causes:
Low blood pressure
Heart Issues
Loss of blood volume
Hypercoagulation (thick blood)
Sticky blood
Inflammation of blood vessels (due to chronic low grade infections — often secondary infections and not primary infections)
Issues with hemoglobin (iron) due to things like chemical pollutants, including carbon monoxide
Each one of these impair oxygen to the brain and thus can cause many symptoms: inability to concentrate, memory issues, mood swings / irritability, light intolerance, noise intolerance, and many many more. Hypoperfusion also occurs with many neurological conditions and forms of dementia.
To add a personal note, during one relapse of ME/CFS my SPECT scan showed significant hypoperfusion which the radiologist read as “possible early onset Alzheimer’s disease”(due to my age) – it was not, I fully recovered (as evidence by some 1500 blog posts on this site and it’s sister site, Microbiome Prescription Blog.
ME/CFS Literature
When patients deal with MDs, having a rich collection of studies often persuade them to take something serious instead of dismissing it as something from the internet rumor-mill. So, I have assembled prior studies below. Note that POTS has been a hallmark of ME/CFS and is associated with hypoperfusion.
In 20+ years reading literature on ME/CFS, the following issues (or a combination) appear to be dominant causes:
Hypercoagulation — David Berg, Hemex labs was the original reported in 1998 (Summary) – I had many in person and phone conversations with him before he retired.
This includes not just thick circulating blood, but also fibrin fragments and deposits that slows the flow of blood
English translation: Not only the wrong weight of motor oil in the body, but the oil filters are clogged!
Low Blood Volume — David Bell (summary) in 1995, who I have also had phone conversations with
There are a few subsets, like those that suffered organophosphate pesticides exposure (2003). Prolonged ME/CFS reduces the size of the brain (I suspect due to prolonged oxygen starvation)
Endothelial dysfunction in COVID– 19 and cognitive impairment]. 2021;121(6):93-99. doi: 10.17116/jnevro202112106193. “The development of endothelial dysfunction in COVID-19 can disrupt organ perfusion and cause a procoagulant state, leading to both macro- and microvascular thrombotic events. Cognitive impairment is a common complication of COVID-19 that develop in acute and delayed periods and is not directly related to the severity of the underlying disease.”
Putting it all together
First, try to get an Appropriate Brain Scan depending on the method of scan, abnormalities would be be found from 14% to 80% of the time. You want the 80% scan — or else you MD will say “it’s in your head” in the alternative meaning 😦 .
Second, it is very unlikely that you can be tested for each and every candidate item above. In some cases, there may not be the expertise available or the testing deemed experimental/for research purposes only — this can be ignored/dismissed by a treating physician (or their supervisor). For myself, I had coagulation testing with Berg (their test suite is available in a few locations). There are almost a dozen makers examined — most MDs and even specialists — will only test for a few.
I have put together a collection of researched pages dealing with various issues:
The secondary infections are harder to deal with — often they can become occult (using Jadin’s term from the Pasteur Institute for Tropical Medicine), that is, they may not be seen in the blood (an oxygen rich environment) but in the tissue (lower oxygen, and even more when they produce metabolites (toxins) to inflame blood vessels (further reducing oxygen) and cause fibrin barriers to block oxygen from red blood cells getting into the tissue. They may also persist in the gut microbiome and never enter the blood system — instead their metabolites enter the blood system.
Personally, I favor the microbiome alteration approach. The goal is to make a hostile environment for these bacteria by starving them of their preferred food and flooding them with what they do not like. I did the Jadin’s antibiotic protocol (multiple rotating specific antibiotics for months) with earlier relapse — but I have been just as successful with microbiome manipulation with later relapses (and an apparent shorter time to recovery).
There is Hope
Given the number of issues, challenges with MDs, etc, I realize that most patients will likely get zero traction from the conventional medical establishment — unfortunately. I view that there is a viable alternative treatment approach because of the availability of direct-to-retail 16s microbiome tests. We know that there are pattern of bacteria shifts seen in CFS/ME and Long COVID. It is likely (at least from personal experience) that correcting these shifts result in reduce symptom severity and number (and even complete elimination). See my personal experience here.
The key is really simple — alter diet and supplements –NOT WITH A FORMA COOKBOOK MODEL from Internet ramblings of others — but explicitly based on your personal microbiome. The suggested changes are generated (for free) by artificial intelligence on Microbiome Prescription using almost 2 million facts harvested from the US National Library of Medicine. The suggestions are unique to you — but should always be reviewed by your medical professional before starting.
The patient has been under a lot of family stress. Stress is known to flare ME/CFS and to also alter the microbiome. One of the typical symptoms seen is an increase of brain fog.
The last sample was taken on Aug 20, 2021 with 20 symptoms entered.
My Usual Flow for Analysis
With the addition of “Consensus Suggestions” getting suggestions become easier. I can do several analysis and then work off the consensus report. This means less mental exertion for ME/CFS patients
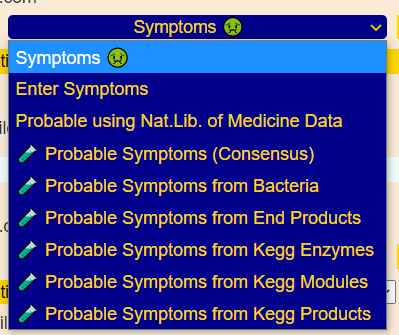
Typically I will start with the top two shown below, but since ME/CFS is included. I have 3 to use
After getting three sets of suggestions by different paths
Takes from Consensus (highest values), there are 130 positive items. I will just pull the highlights.
The flip side — the avoids — often this is hard for ME/CFS to implement. Often they are limited to choices due to available income or other issues (for example histamine issues). Occasionally, they have been convinced to need a specific type of diet.
Diet Style (often people get sold on specific diets as cure-alls)
First, I checked the medical conditions from the new site, GMRepo, and ME/CFS is not listed. This means that any researcher who have done a study, had not contributed their data there 😖. Going to the full list and seeing if anything sticks out for the latest sample there was nothing, there was a weak possibility for (Obesity, Morbid and Clostridium Infections).
Next, I looked at Symptom Forecasting
The predicted symptom really looked like ME/CFS, as shown below
Consensus Prediction of Symptoms
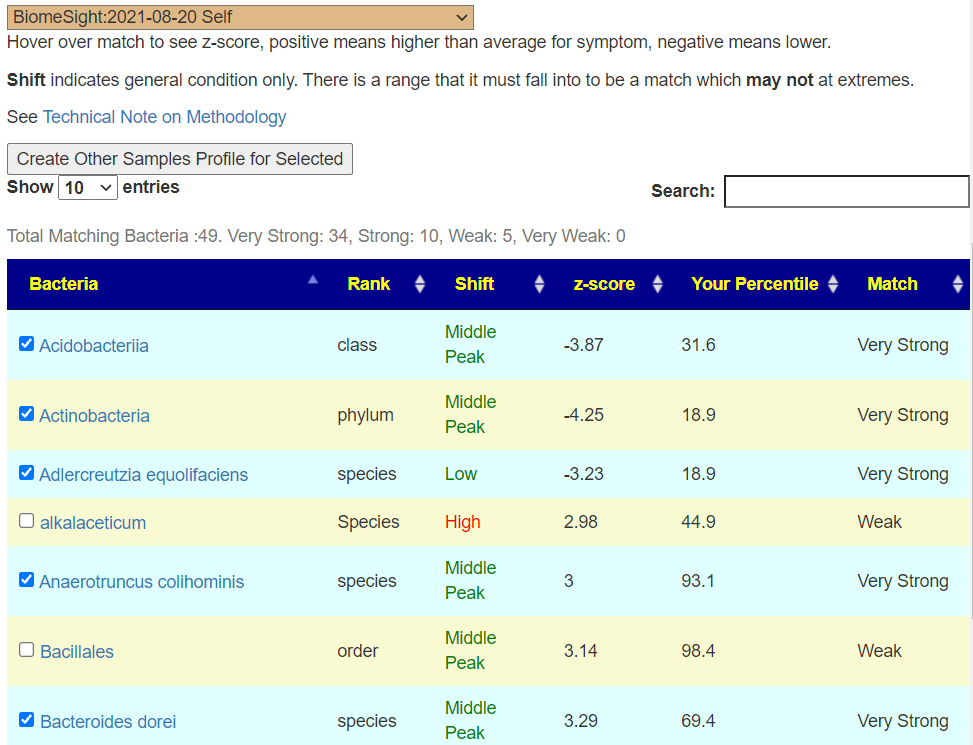
Reducing Salicylates in the diet would be an additional suggestion. I clicked on the top item, DePaul University Fatigue Questionnaire : Difficulty following things especially since the person reported more severe brain fog recently.
This takes me to a page showing the bacteria involved. We have 44 out of 49 bacteria having a strong or better match.
We then create an additional sample profile by clicking the [Create Other Samples Profile…] , view the suggestions and returned to the consensus page (which now uses all 4 suggestion list)
beta-alanine – which appears to be execrated more in ME/CFS [1996] “Increased excretion of beta-alanine was found in a subgroup of CFS patients, indicating that there may be a link between CFS and beta-alanine in some CFS patients.” [2007]
Proline — “The disorder of arginine-proline metabolic pathway is detected in CFS middle school students before exercise intervention.” [2018]
There were also some items that I could not find any suitable literature on and thus I am ignoring.
Bottom Line
This has been a pro-forma walkthru of how to analysis the microbiome of a person with ME/CFS. We used several different approaches to get multiple sets of suggestions which we viewed in the Consensus Report. Each way used a different model of which bacteria to select (since no one knows the right one that works for everyone!).
Looking at the items above, my personal high priority choices would be to go hard on stress reducers:
Mutaflor or Symbioflor-2, with D-Ribose to provide food for it.
And then the appropriate items on the above lists.
REMEMBER — do not ignore the Avoid list. Doing so will reduce or eliminate the benefits from the Take list.
As always, this is not medical advice — all suggestions should be discussed with a knowledgeable medical professional before starting. This is a walkthru of using an academic model (not based on clinical experience) to model what may improve the microbiome examined. Every microbiome is unique and the contents of this post cannot be applied to other people.