I saw a comment on a post claiming that chelation is all that is needed. Really? I have heard that same claim being made for over 25 years — so what is the peer review evidence.
“The recognition of these processes implies, mechanistically, that therapeutic benefit is potentially to be had from antioxidants, from anti-inflammatories, from iron chelators,” [2022] No evidence, just hypothesis
Part of an extensive treatment, those that did everything improved. [2013]
“The reactivity of lymphocytes to metals declined after dental metal removal, and 83 patients (76%) showed long-term health improvement, 24 patients (22%) showed unchanged health and two of them (2%) showed worsening of symptoms ” [2006]
A definitive study
The paper below found no evidence of systematic high levels of minerals for people with ME/CFS.
Labs do not show evidence supporting a need to have chelation. There are no studies showing that it is effective — yes, there is speculation but after over 30 years the absence of study evidence is pretty condemning for it.
People may improve — yes! It is called the Placebo effect, and you can get real improvement from the placebo effect. How? Believing that it will work will reduce your stress levels and thus improves the microbiome.
For those that claim that it helps “Show me the peer review studies!” I work on gold standard evidence not what Jack told Jane based on what Sue told her.
In 1994, after two years of a high stress job managing and motivating direct sales groups in my own sales company I quit and I spent 6 months very fatigued, without moving my body very much and staring at the void sitting on my sofa. I could barely lift a glass of water. After the six months I regained strength and I commenced in a new job. Doctor said I had the yuppie flu, gave some vitamins and tests showed I had had epstein-barr viruses.
In 2008 I recall being very fatigued again. And again 6 months secluded at home sleeping 14 hours a day (I have no family in Spain). I could work but I was uneasy and the job was stressful at times,. In 2009 I started to undergo tests in a private clinic, cause the public hospital who was cutting edge at CFS has a a waiting list of years. I wanted to know what I had. Blood samples, screening, mutaflor, some other immune system boosters, etc. Diagnosis 2010: CFS (not Fibromyalgia yet). I started also to attend to conferences and read a lot about my illness (which I don’t do anymore).
In 2016, after years working with fatigue and pain I decided I couldn’t stand it anymore and thought I should care about myself so I went on sick leave for one year. Afterwards I solicited voluntarily leave of absence.
CFS/EM slowly shifted more to Fibromyalgia. I was diagnosed in one of the best public Hospitals in Barcelona (the renowned Hospital Clínic). They gave me advice on doing exercise, not much more.
Now I say I have moderate EM and moderate to severe Fibromyalgia. Depends on the day. I stay at home mainly. IBS, Psoriasis, Costocondritis sometimes, eye problems, dizziness. muscular problems and stiffness, etc. I am going to a Quiropractic for many years. With an electric bike I can do some miles.
I see there are a lot of supplements in Biomesight, It would be highly appreciated if you could give some insight of my Biomesight results and how to get started changing my gut’s microbiome (food, supplements, etc).
Clarity on Suggestions from Biomesight
I do not know how Biomesight derive their suggested supplements. Many microbiome providers use nutritionists who often suggest generic “healthy” supplements. In other cases, they have found a study for a supplement that impacts one bacteria and if you are high or low for that bacteria, suggest that (ignoring what that same supplement will do to other bacteria!). I would love to see a detailed blog from Biomesight on how they determine appropriate supplements to suggest.
Microbiome Prescription uses almost 1.9 million facts(i.e. X substance modify Y bacteria) and then consider all interactions that a supplement has on all bacteria of concern.
Analysis
First, we will look for a common fingerprint for ME/CFS and Long COVID: Over representation of bacteria in the 0-9%ile. We have a very strong match shown below. The numbers in each range should be about the same number for a healthy microbiome.
Looking at Dr. Jason Hawrelak Recommendations we find it at 75.3%ile, indicating issues with the following being most concerning:
Faecalibacterium prausnitzii well below his low limit. This bacteria is deemed anti-inflammatory [2008] and thus a contributor
The Potential Medical Conditions Detected using the US Library of Medicine studies show what you reported and a few other items of concern (Asthma, Colorectal Cancer [possible false positive], etc)
Fibromyalgia 96%ile
Chronic Fatigue Syndrome 96%ile
Inflammatory Bowel Disease 94%ile
Gastroesophageal reflux disease (Gerd) including Barrett’s esophagus – 97%ile
Going Forward
First a quick video on the process
I did the “Just give me suggestions” followed by individual sets of suggestions for the four above item resulting in 8 sets of suggestions done with different criteria to select critical bacteria (See video). We then use consensus to identify the items most likely to help. This is a way to improve results in the face of many unknowns.
Probiotics (usually I suggest take 1 probiotic for 2 weeks at sufficient dosage (see this supplement dosages link) and then rotate to the next one on the short list, then repeat.
Antibiotics (if you have a willing MD) — one course then 3 weeks off, then a course of a different one. All of the ones below has been used by specialists for ME/CFS or FM
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
The earliest use of antibiotics for treating ME/CFS that I am aware of, dates from the late 1990’s with articles in Journal of Chronic Fatigue Syndrome (and conference reports prior)
My remission from ME/CFS was done by combining C.L. Jadin protocol with Dave Berg anticoagulant protocol.
Overview of results
First, let us show the numbers and then talk about them. It is clear that there are significant changes. There are a lot of dimensions to consider.
Criteria
2-Mar
9-Mar
21-Mar
3-Apr
16-Jun
Shannon Diversity Index (Percentile)
85.2
79.0
99.8
72.4
16.0
Simpson Diversity Index (Percentile)
72.6
63.4
64.4
77.0
91.4
Chao1 Index (Percentile)
65.7
31.2
77.2
62.9
7.9
Lab Read Quality
8.9
8.7
6
4.5
4.4
Bacteria Reported By Lab
654
533
725
585
389
Bacteria Over 99%ile
2
4
30
11
24
Bacteria Over 95%ile
13
10
70
33
38
Bacteria Over 90%ile
25
23
103
63
55
Bacteria Under 10%ile
287
213
123
113
140
Bacteria Under 5%ile
253
173
66
48
96
Bacteria Under 1%ile
219
135
17
8
46
Lab: BiomeSight
Rarely Seen 1%
13
1
38
5
6
Rarely Seen 5%
28
9
107
17
29
Pathogens
36
31
50
40
36
Outside Range from JasonH
6
6
9
9
8
Outside Range from Medivere
15
15
22
22
22
Outside Range from Metagenomics
7
7
9
9
9
Outside Range from MyBioma
5
5
6
6
6
Outside Range from Nirvana/CosmosId
26
26
18
18
15
Outside Range from XenoGene
28
28
46
46
42
Outside Lab Range (+/- 1.96SD)
6
8
56
17
27
Outside Box-Plot-Whiskers
44
36
124
70
67
Outside Kaltoft-Moldrup
233
169
207
137
170
Condition Est. Over 99%ile
0
0
13
10
48
Condition Est. Over 95%ile
1
0
24
35
75
Condition Est. Over 90%ile
2
2
34
55
84
Enzymes Over 99%ile
0
0
347
606
957
Enzymes Over 95%ile
7
0
635
970
1145
Enzymes Over 90%ile
24
28
746
1159
1228
Enzymes Under 10%ile
506
515
561
237
245
Enzymes Under 5%ile
378
360
422
143
174
Enzymes Under 1%ile
194
166
120
52
94
Compounds Over 99%ile
0
0
225
215
617
Compounds Over 95%ile
2
0
355
410
732
Compounds Over 90%ile
8
11
441
520
778
Compounds Under 10%ile
1243
986
1105
902
822
Compounds Under 5%ile
1156
926
1032
856
796
Compounds Under 1%ile
1115
875
936
828
767
Next are the percentages by percentile which I noticed tend to have over representation with ME/CFS and Long COVID in the 0-9 percentile. We see this pattern at the start, with improvement and then a bounce back to high numbers.
2-Mar
2-Mar
9-Mar
9-Mar
21-Mar
21-Mar
3-Apr
3-Apr
16-Jun
16-Jun
Percentile
Genus
%
Genus
%
Genus
%
Genus
%
Genus
%
0 – 9
65
40%
51
36%
28
15%
29
19%
35
36%
10-19
13
8%
16
11%
36
19%
23
15%
9
9%
20 – 29
11
7%
16
11%
20
11%
23
15%
14
14%
30 – 39
5
3%
9
6%
17
9%
17
11%
4
4%
40 – 49
13
8%
10
7%
14
8%
11
7%
5
5%
50 – 59
12
7%
8
6%
10
5%
8
5%
3
3%
60 – 69
12
7%
9
6%
6
3%
14
9%
1
1%
70 – 79
12
7%
3
2%
10
5%
6
4%
5
5%
80 – 89
10
6%
10
7%
15
8%
9
6%
7
7%
90 – 99
11
7%
8
6%
30
16%
15
10%
15
15%
Total
164
140
186
155
98
2-Mar
2-Mar
9-Mar
9-Mar
21-Mar
21-Mar
3-Apr
3-Apr
16-Jun
16-Jun
Percentile
%
Species
%
Species
%
Species
%
Species
%
Species
0 – 9
41%
94
43%
79
13%
40
17%
36
21%
31
10-19
6%
14
9%
16
15%
44
13%
28
9%
13
20 – 29
8%
18
9%
16
13%
39
12%
27
15%
22
30 – 39
3%
7
5%
10
10%
29
10%
22
8%
11
40 – 49
7%
17
4%
7
7%
20
8%
17
6%
9
50 – 59
9%
21
5%
9
7%
22
6%
12
5%
7
60 – 69
6%
14
8%
14
3%
10
6%
14
6%
9
70 – 79
8%
18
4%
7
6%
19
7%
15
6%
9
80 – 89
6%
13
8%
15
8%
23
8%
17
10%
14
90 – 99
5%
12
6%
11
19%
57
13%
29
14%
21
Total
228
184
303
217
146
The Events Around the above Samples
2023-03-02 (baseline)
2023-03-09 (during a stomach bug)
2023-03-21 (during a “Level 1” remission while taking Amoxiclav. Level 1 = all symptoms gone. Felt great. Had started Amoxiclav on the morning of 3/20, this sample was taken after 3 doses around 3pm)
2023-04-03 (4 days after stopping Amoxiclav, was on Doxycycline)
2023-06-16 (During 2nd round of Amoxiclav when I felt really bad)
The microbiome results definitely reflected the Level 1 remission on 3-21. The low percentile genus and species percentage almost made it to the target level of 10% from the prior 40%! The Shannon Diversity Index was awesome (the higher the better!).
I have often described correcting the microbiome as being similar to sailing a sailboat along a coast line. Depending on wind and tide, there may be a lot of course changes required. I am curious on the ranking of Amoxiclav[amoxicillin] and Doxycycline with these samples. The numbers below suggests that going on to Doxycycline may have been a poor choice. On the 2nd round of Amoxiclav, it was at just 35% of the highest value recommendation versus 70% on the 1st round.
Note that rifaximin and rifampicin are in the same family and used by some ME/CFS specialists. Imipenem shows up often with ME/CFS samples — but since it is intravenous, not the easiest to get on an ongoing basis.
Take Away and Reflections
This project main purpose was to show that remission can be triggered by antibiotics to another generation of people suffering from ME/CFS. The remission on 21-Mar demonstrates this to be correct both subjectively and objectively (Microbiome data — specifically Shannon Diversity Index and Percentages in different percentiles for Species and Genus). I should emphasis that both of these measures are multi-bacteria measures and do not support the common myth that ME/CFS is caused by a single bacteria.
The critical issue is maintaining remission. How do keep the microbiome where it should be. I often use analogies of cities because we are talking about a city of bacteria. To stop riots and looting in the streets you send in the National Guard (antibiotic). The city is back to normal. The causes of the the riots are still there. Typically lack of opportunities, neglect, etc. in these same ghettos. You must address these other issues. A repeat of sending in the National Guard may have the same effect as the first time OR very different effects – the same can be said for using the same antibiotics.
With bacteria we have two “radical organizations in the ghetto” — The Antibiotic resistant and the Resistors. For example, the bacteria that survive learnt how to avoid the National Guard and proceed to share that skill to other bacteria. Instead of a wall of shields pushing the rioters back, Molotov cocktails rain down on the troops from above.
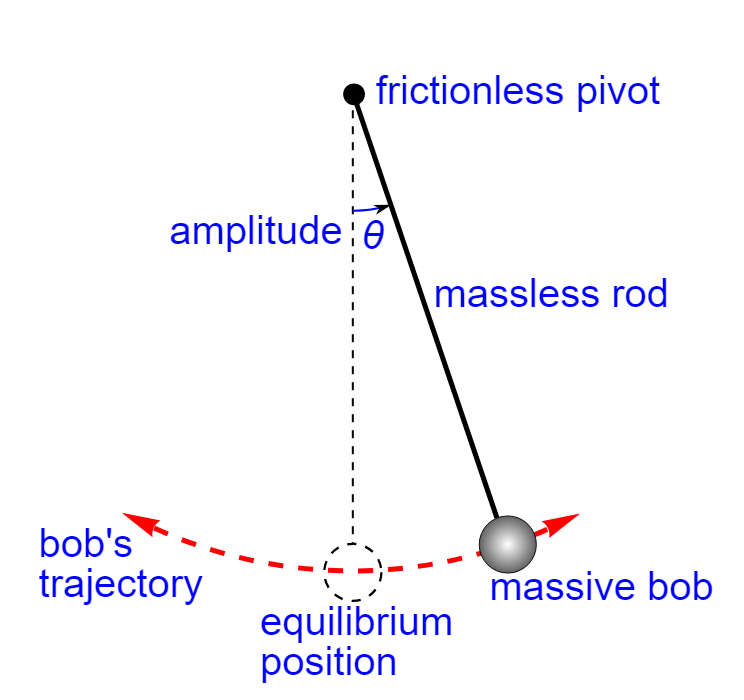
Another analogy is that the gut is a pendulum. The antibiotics, probiotics and other items pushes the gut towards the equilibrium position! There is great joy! The gut is centered… At this point, many people go down the wrong reasoning path — “Keep doing more of the same to stay in remission!“. Remission is lost and the momentum pushes the guts out to the other side!!! You pushed out one devil and seven more devils return! (Math 12:43-45)
The key is to dampen down the swing so there is less and less swing. My personal opinion is that Cecile Jadin’s protocol using antibiotics for only 7 days each month is a very effective way of dampening the pendulum gained from decades of experience.
My approach with Microbiome Prescription is to try to address the whole city. Before taking action, we get intelligence on the nature of the city and decide on the appropriate action for a period of time (typically 4-10 weeks). We then update our intelligence (i.e. microbiome test) and pick the next course of action. Actions may include “food kitchens”, “safe injection sites”, “training programs”, “home repairs”, “on the beat policing”, etc.
There are many people who will state that antibiotics gave me ME/CFS. I do not disagree. Antibiotics can also trigger remission — the problem is WHICH antibiotics. Since every person’s microbiome is unique, there can be no universal “best antibiotic” for ME/CFS. Antibiotics must be selected based on the individuals microbiome (which is the path that Microbiome Prescription took) for the best odds of making the right choice.
My Suggestions Going Forward
I am working with C.L. Jadin, M.D., on documenting her current protocol from almost 30 years of experience using antibiotics for ME/CFS. It will be out soon. I am hoping to have that available within a month. One key aspect of her protocol has been pulsing antibiotics using two at a time. There are a few studies showing that pulsing is more effective. Pulsing often means 7 days on and 21 days off.
Looking at Tess’s last sample, I would propose the following to be considered (items that I picked from the consensus suggestions):
Take a 3 week break from antibiotics (Ideally at the end take another sample)
A common pattern of people is “Just give me a pill to fix me, I want to keep my current life style and I am not prepared to make significant life style and diet changes”. My impression is that making those changes is often required. Inertia is a real maintainer of ME/CFS, especially the pendulum inertia when trying to heal.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide information on rotations etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
People who have read my blogs over the last few decades know that I keep to direct evidence; I avoid speculation and “I figure things work this way” thinking. Microbiome tests is a key part of it. My preference is to get as much data as is affordable/reasonable. This is typically my Bacteria Reported/Cost ratio. At the moment, Thorne is the distinctive winner.
Another data source can be smart watches. I have written about this in the past, Monitoring watch for CFS and other Conditions [2021]. After two years, my watch suffered failure on the charging toggle; so time to get a new one — what I got is described below. Every year features increases on smart watches. My first watch took only a few measurements and only on the hour.
Not Prestige Watches
I could go Apple Watch ($400), Fitbit ($300), Samsung ($450) etc. and drop a few hundred dollars for a device that will likely be technologically obsolete in 2 years. Or go with a Chinese model that costs $40 and which will last 2 years or more. In many cases, the key sensors may be the same as used in the prestige models. In some cases, these Chinese watches have features not available on the prestige watches.
Accuracy/Medical Grade is NOT the purpose
I use the watch to detect differences. In general, I find the results are reasonably accurate when I compare to standalone devices.
For most people (especially those with brain fog), their memory is poor and often they do not feel there was any change based on subjective memory. Having daily history going back months allows you to get objective measurements of things that change. Hopefully, it will stop you from ceasing something that is actually helping. Remember, I am very objective evidence based.
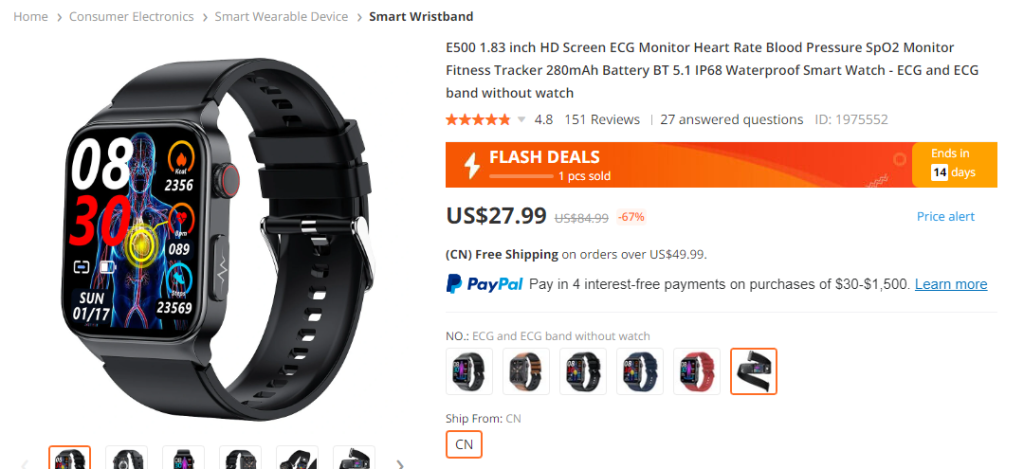
Review of my latest watch
You can find them on Temu or Banggoods. My model is E500. Once I got mine, my wife wanted to upgrade to the same model and did.
The screens
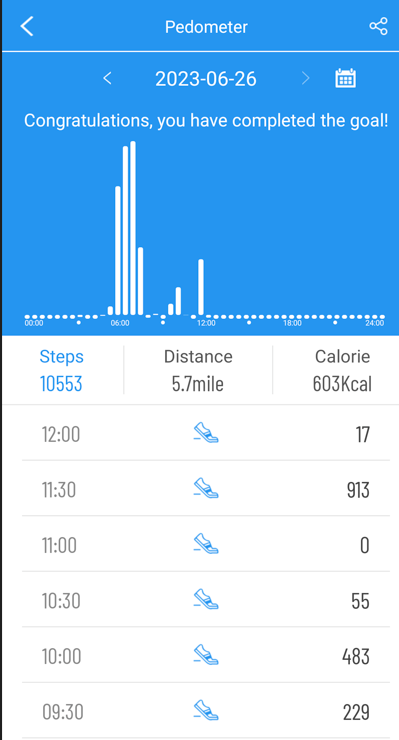
How many steps today and hours of sleep with details below
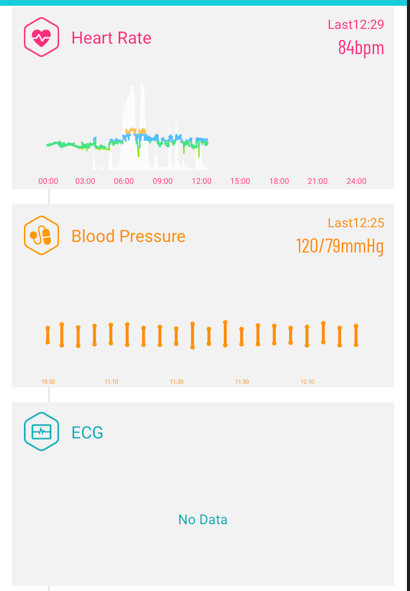
Then Heart Rate, BP and ECG (manually done)
Some Drill Down Details
Sleep Quality is often influenced by the Microbiome
Having daily detail breakdown is sweet!
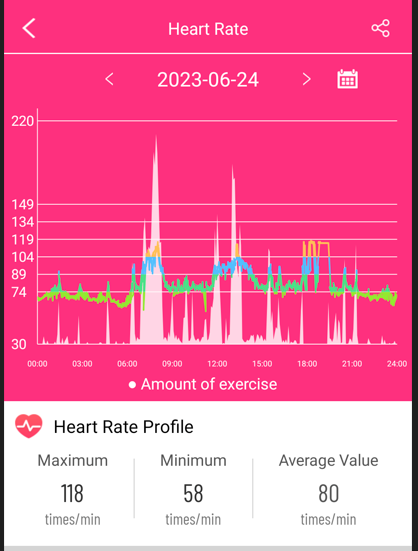
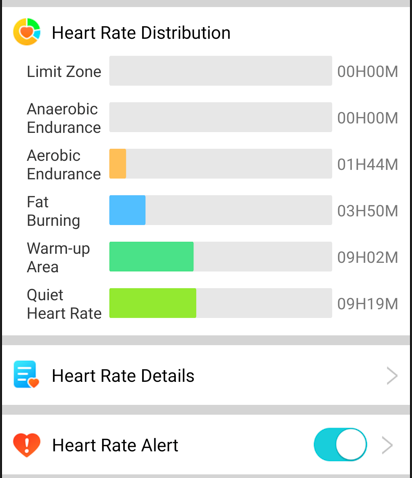
The heart rate also maps activities (such as steps) providing better understanding!
With a good summary
Blood Pressure is every 5 minutes. With the other data, if there is a spike, you have enough other measurement to evaluate the events and causes.
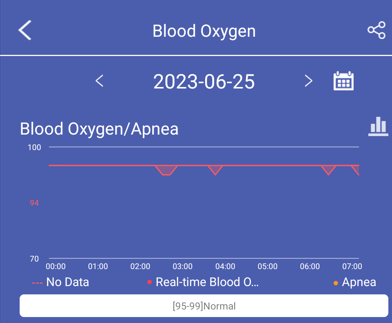
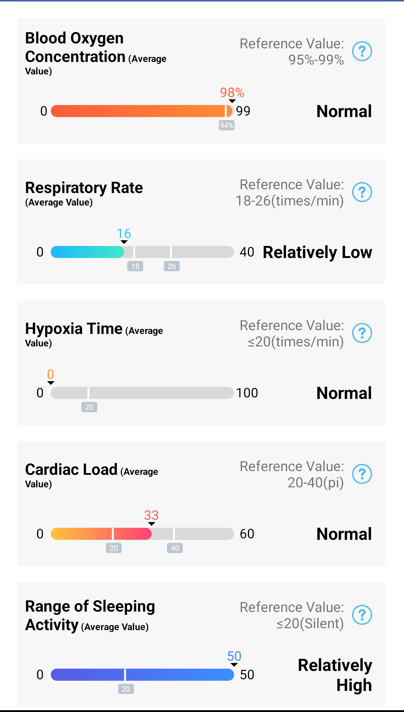
Oxygen Measurement is far better than a finger device!
And more details
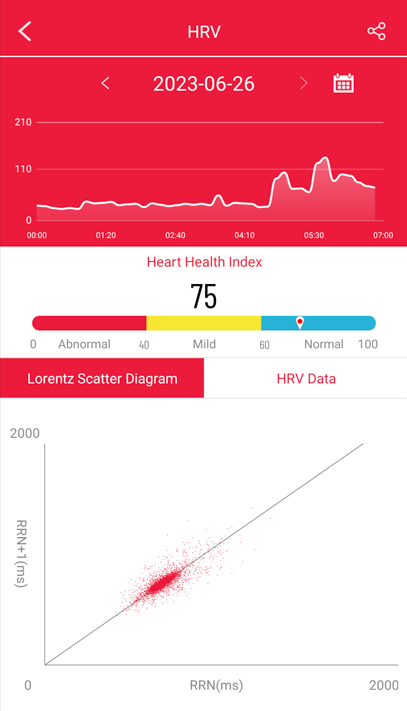
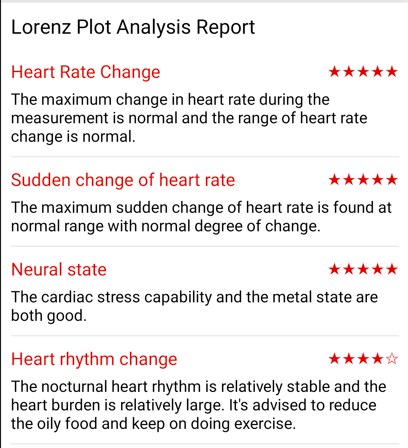
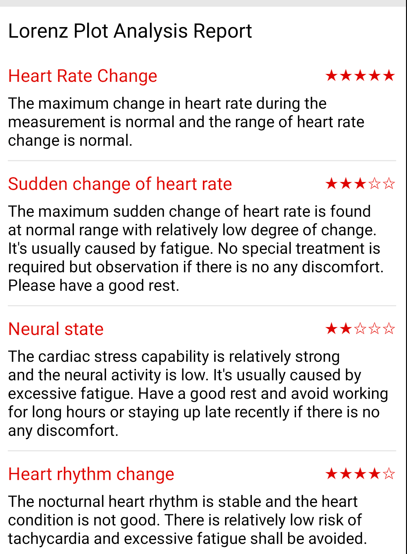
HRV – Heart Rate Variability
With simple summary and ratings
Below is an example from a day that I was pushing myself for physical activity more than usual (some who use the term “out of shape”). Fatigue was definitely happening!
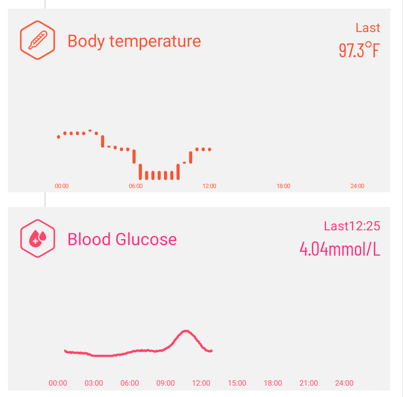
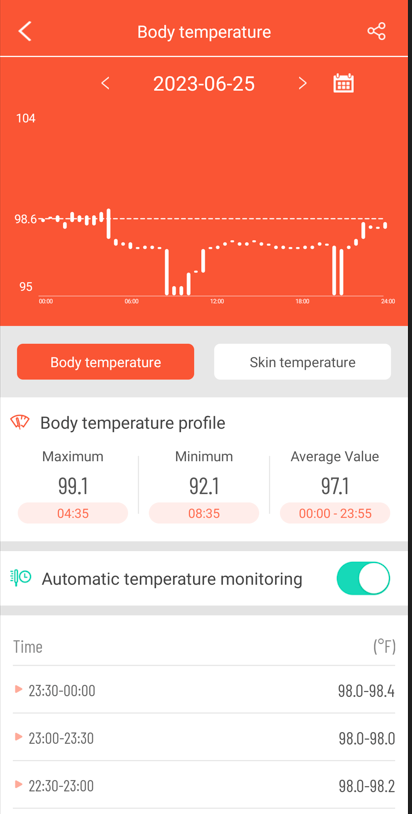
Night Sweats
At present, I do have night sweats — the temperature monitor definitely show it. They start about 3 hours after going to bed and stops when I wake. As is common for people with ME/CFS (including those that are recovered), I have below normal temperatures.
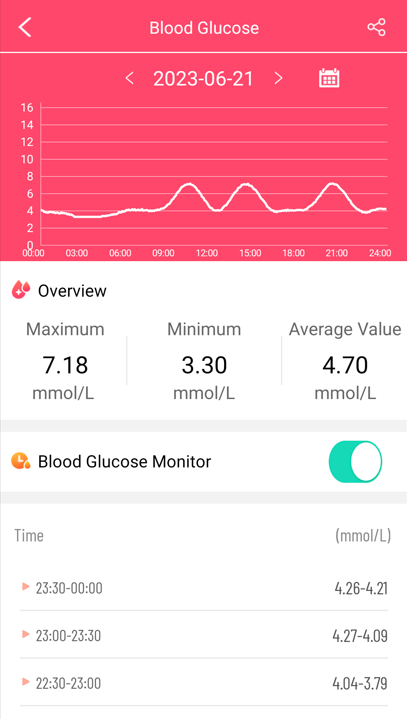
Blood Glucose Levels
This can be very good to determine how well your meals are handled by your body
Bottom Line — Concrete, Detailed Objective Data!
There is a little overhead. I usually do periodic screen captures on my phone and off load the images to my PC so I can compare what was to what is.
I’ve had bloating and burping since hospitalized as a child for a lump on my throat. I received antibiotics at this time
I went into 80% remission for about 6 years from age 50-56. I don’t know what did it but I was on a low FODMAPS diet and started using hydrogen peroxide as a mouth rinse
Symptoms
in addition to the bloating and burping I have the following symptoms
fatigue
sometimes a numb feeling in parts of my hands and feet
orthostatic intolerance (although I did the tilt table test and tested negative)
halitosis
tinnitus
a strange feeling in my head
shortness of breath
I took inulin before my remission and my symptoms intensified immensely (especially burping and fatigue and shortness of breath)
I had a culture of my upper duodenum done in 2013 and it showed 10000CFU/ml of rothia, prevotella melaninogenica and streptococci viridins. A recent Bristle Health oral biome test showed the prevotella melaninogenica in the 90th percentile
Analysis
I was not surprised about getting ME/CFS after a cold. Cold virus include COVID which can cause Long COVID — a sibling of ME/CFS. The wrong cold virus combined with other catalysts can send someone down that path.
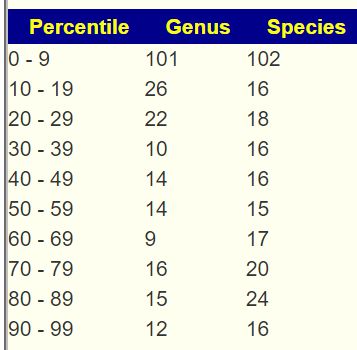
First, I look at the distribution of percentiles. A normal/typical microbiome should have the same count (percentage) in each of the 10%ile. As is often seen with ME/CFS and Long COVID, we have a major overrepresentation of the 0-9%ile — 4x the count of most other groups.
Percentile
Genus
Species
0 – 9
62
89
10 – 19
14
22
20 – 29
15
22
30 – 39
16
16
40 – 49
15
19
50 – 59
20
25
60 – 69
10
14
70 – 79
18
22
80 – 89
20
17
90 – 99
21
35
I interpret this as a host, “a mafia”, of odd bacteria that cross support each other and pumps disrupting metabolites (chemicals) into the body. Thus it is not a bacteria(person) that causes the problems but a big gang of bacteria.
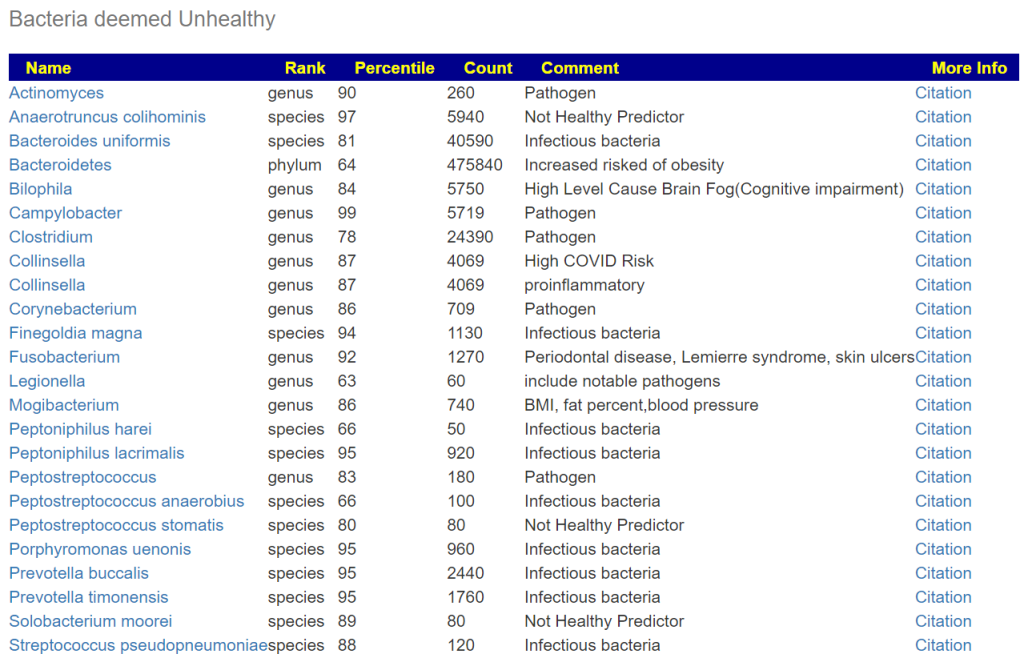
There was not a strong bacteria that predominate this shift, Phocaeicola massiliensis was the only candidate. Looking at Potential Medical Conditions Detected, there were no significant matches (not surprising with an abundance of low percentile bacteria).
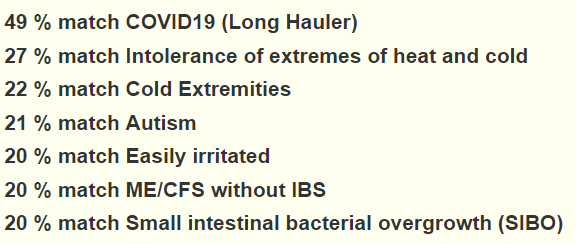
Looking at some of the conditions we see a marginally better match for Long COVID than for ME/CFS! Not sufficient to ascribe to a cold virus as the onset cause, but interesting.
It provides information on selected strains by role:
As an exercise to understand the “end-to-end” process (literally), I have created the table below. Since the data is by species we have an issue of different tests reporting different species. For more details see The taxonomy nightmare before Christmas… The * indicate that there was no match at the strain level, so we use the genus as a proxy.
First thing to remember is that bacteria is pH sensitive so the quantity in each location is expected to be very different.
Bacteria
Bristle
Percentile
Actinomyces dentalis
1.8
90
*
Actinomyces graevenitzii
1.9
90
*
Actinomyces odontolyticus
0.4
90
*
Atopobium parvulum
6.8
69
*
Atopobium sp
8
69
*
Campylobacter concisus
5.2
98
*
Campylobacter gracilis
5.1
98
*
Candida albicans
1.8
Candida dubliniensis
1.5
Candida glabrata
2.2
Candida sp
1.1
Capnocytophaga granulosa
7.3
Capnocytophaga sputigena
0.19
*
Capnocytophaga sp
0.18
*
Corynebacterium matruchotii
8.3
86
*
Dialister micraerophilus
0.4
94
*
Eikenella corrodens
2.6
Enterobacter cloacae
2.5
Fusobacterium nucleatum
1.9
19
Fusobacterium sp
0.3
92
Gemella haemolysans
1.8
48
*
Gemella morbillorum
0.12
48
*
Granulicatella adiacens (30%)
4.8
15
Haemophilus haemolyticus
4.8
Haemophilus parainfluenzae
7.2
Haemophilus pittmaniae
0.79
Helicobacter pylori
2.3
61
*
Lactobacillus fermentum
3.5
5
*
Leptotrichia trevisanii
0.99
Megasphera micronuciformis
8.5
24
*
Neisseria elongata
0.15
*
Neisseria flavescens
2.1
Neisseria mucosa
3
Neisseria subflava
1
Oribacterium sp
0.098
26
Porphyromonas sp
2
100
Porphyromonas catoniae
0.27
100
*
Prevotella sp
10
73
Prevotella fusca
2.2
73
*
Prevotella histolica
9.5
73
*
Prevotella loescheii
1.6
1
Prevotella melaninogenica
9
73
*
Prevotella pallens
0.1
73
*
Prevotella salivae
8.8
73
*
Prevotella tannerae
0.56
73
*
Prevotella veroalis
7.5
73
*
Propionibacterium acidifaciens
2.1
Rothia aeria
0.8
Rothia mucilaginosa
5.2
Selenomonas noxia
4.4
72
*
Solobacterium moorei
0.3
89
Stomatobaculum longum
0.18
Streptococcus constellatus
2.7
48
*
Streptococcus infantis
7.9
48
*
Streptococcus intermedius
1.9
0
Streptococcus mitis
7.8
48
*
Streptococcus oralis
7.2
1
Streptococcus parasanguinis
1.3
49
Streptococcus peroris
1.6
48
*
Streptococcus salivarius
5
48
*
Streptococcus sanguinis
2
48
*
Streptococcus tigurinus
8.7
48
*
Tannerella sp
0.88
Treponema sp
0.73
Veillonella atypica
8.5
18
Veillonella dispar
7.5
18
*
Veillonella sp
2.7
18
*
I noticed something interesting with strains that were in both samples.
My subjective conclusion is that this strongly supports the hypothesis that the mouth microbiome feeds the microbiome of the rest of the digestive track. We have 4 rare strains in the above list of 7 where only 1 would be expected to be below 14% (1 in 7).
We can get suggestions for the mouth approximately by using this feature and entering by the genus items above 7 for high, 9 for very high or below 3 for low, below 1 for very low.
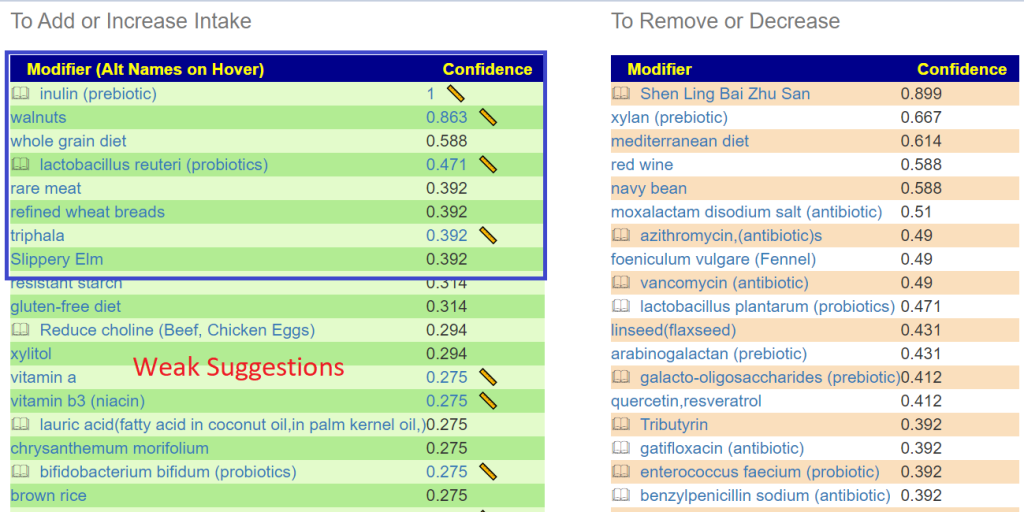
Suggestions include (for mouth) are below. This is an experiment to see how suggestions for the “other end” compares! Values below 0.4 are usually low significance.
There are some subjective issues in entering the contents and getting suggestions. For suggestions, doing parent and/or children of a bacteria can be debated many ways. Some species are low of a genus and others are high… do you mark the genus high, low or normal? It is unclear if the bacteria listed are pure bad or just bad in excess. That is, should anything not zero be deemed too high or only those over 7. Things are not sufficiently cleared from this report. If I get more requests to do analysis of Bristol Health reports, I will invest more time and add a custom manual entry page. I will need to research every single species to know the appropriate handling.Below is for purposes of illustration only
The adage “No man can server two master” is good to keep in mind in this scenario.
I did the usual “Just Give Me Suggestions” path since there was nothing that stood out that could require special handling. “Just Give Me Suggestions” obtains 4 sets of suggestions using different logic to try to derive the best suggestions. I will start by taking the above list and see how they rank in terms of the microbiome.
As expected, with my two masters preamble, we have disagreements. All of the mouth items came in as weak suggestions against BiomeSight suggestions (range: -460 to 465), so doing them will likely not have significant impact on the other end’s microbiome.
Back to Microbiome Suggestions, we have in decreasing priority (excluding antibiotics):
Looking at Diet Styles, only two are strong indicated, both avoids (listed above).
Food Site
The food site takes the nutrients found and assists in building a food menu plan.
The top Nutrients Suggested
For the top one, a nutrient unfamiliar to most people, we see this list to choose from. We See Barley on it. It Barley is a problem, then almond, peanut or pistachio are good alternatives. For Peanuts, I actually did some posts in the ME/CFS context.
Hesperetin is in Lime, Blond Orange, Lemon and Grapefruit (AGAIN Grapefruit!)
Questions
Q: On cfsremission and/or cort johnsons blog you discussed the importance of breaking down biofilms with things like nac as well as rotating herbs, probiotics and antibiotics. Is that a layer that should be added onto the items selected by microbiomeprescription (I plan to reread those posts before starting).
A: Yes, I have posted about biofilm in the past: Combating an Infection Defense Mechanism: Biofilms [2014] and Probiotic Biofilm Breakers[2016]. It is not a simple matter “Biofilms provide survival sites for both beneficial and opportunistic pathogenic bacteria, by providing protection as above and increasing the potential of the bacteria to survive and evolve” [2013]. It impacts antibiotic resistance [2020]. In other words, we have yin-yang. If you are intending to aggressively reduce bacteria known to use biofilms, especially with antibiotics, then it is a wise choice. In most cases, I would not do it by default. For example, Akkermansia muciniphila and Lactobacillus rhamnosus GG both form biofilms [2020].
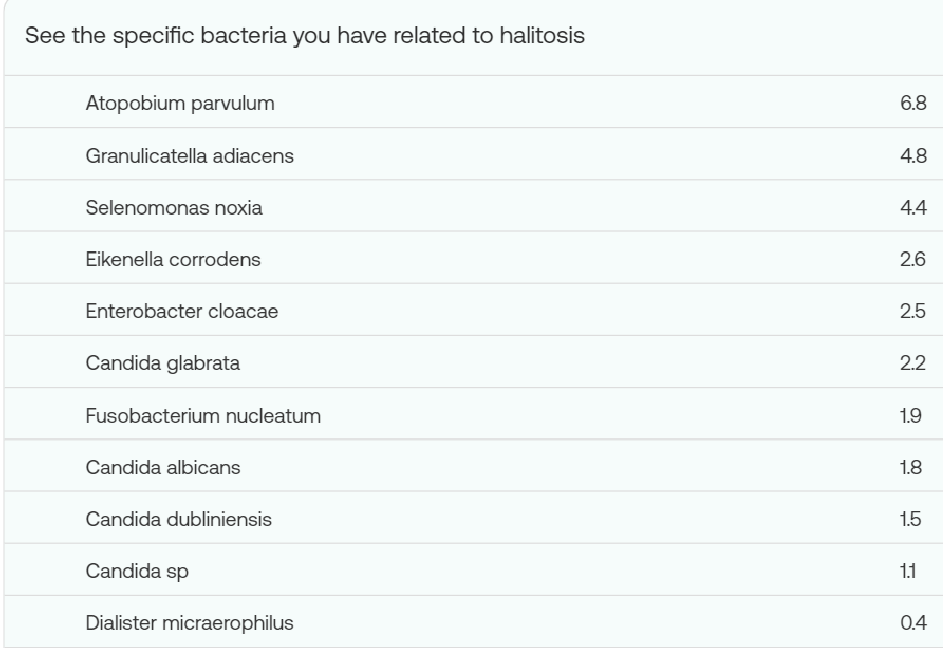
Q: What can you suggest to deal with Halitosis (Bad Breath)
A: The bacteria involved are nicely listed in your report.
In the resulting list we see many items that can be used as teas (which would likely impact the mouth bacteria): triphala, oregano (origanum vulgare, oil) . Items that can be chewed in the mouth: mastic gum .
The same approach may be done for other mouth bacteria that you wish to eliminate, you should cross check that none of the substance are strong avoid for the “other end”.
“The detrimental effects of oral microorganisms are not confined to the oral cavity, they can also contribute to systemic disorders, such as type 2 diabetes mellitus, cardiovascular disease, and inflammatory bowel disease (IBD) (Hajishengallis and Chavakis, 2021). “
“In the article by Chen et al. the influence of periodontal pathogen infection on gut mycobiome was explored. The authors demonstrated the first evidence of gut fungal dysbiosis with periodontal pathogen administration. “
The oral microbiome impacting the entire flow (including SIBO) seems to be well illustrated with this data. The bacteria strains from the Bristle Health report appear to be those known to cause issues in the mouth (and most are not reported on by other tests). This implies that the ideal pair of tests to deal with systemic health issue is likely Bristle Health and Thorne.